

Prevalence, Characteristics, and Outcomes of COVID-19-Associated Acute Myocarditis
- PMID: 35404682
- PMCID: PMC8989611
- DOI: 10.1161/CIRCULATIONAHA.121.056817
Prevalence, Characteristics, and Outcomes of COVID-19-Associated Acute Myocarditis
Abstract
Background: Acute myocarditis (AM) is thought to be a rare cardiovascular complication of COVID-19, although minimal data are available beyond case reports. We aim to report the prevalence, baseline characteristics, in-hospital management, and outcomes for patients with COVID-19-associated AM on the basis of a retrospective cohort from 23 hospitals in the United States and Europe.
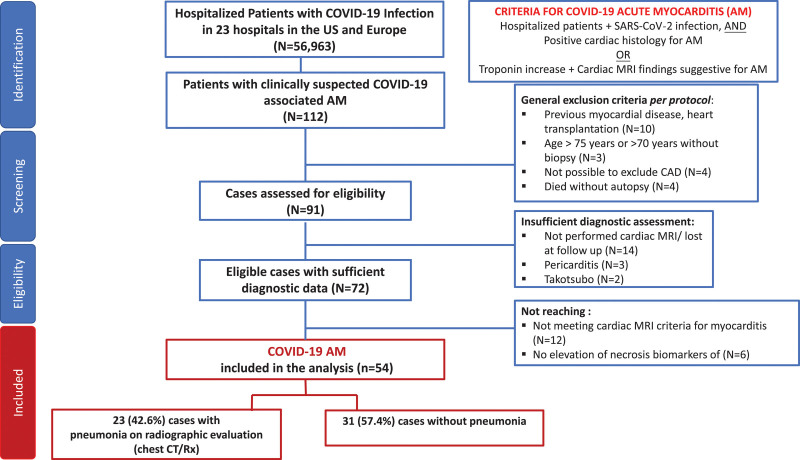
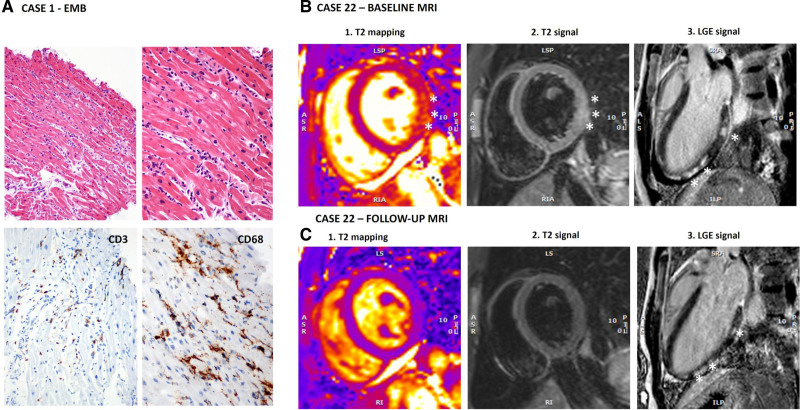
Methods: A total of 112 patients with suspected AM from 56 963 hospitalized patients with COVID-19 were evaluated between February 1, 2020, and April 30, 2021. Inclusion criteria were hospitalization for COVID-19 and a diagnosis of AM on the basis of endomyocardial biopsy or increased troponin level plus typical signs of AM on cardiac magnetic resonance imaging. We identified 97 patients with possible AM, and among them, 54 patients with definite/probable AM supported by endomyocardial biopsy in 17 (31.5%) patients or magnetic resonance imaging in 50 (92.6%). We analyzed patient characteristics, treatments, and outcomes among all COVID-19-associated AM.
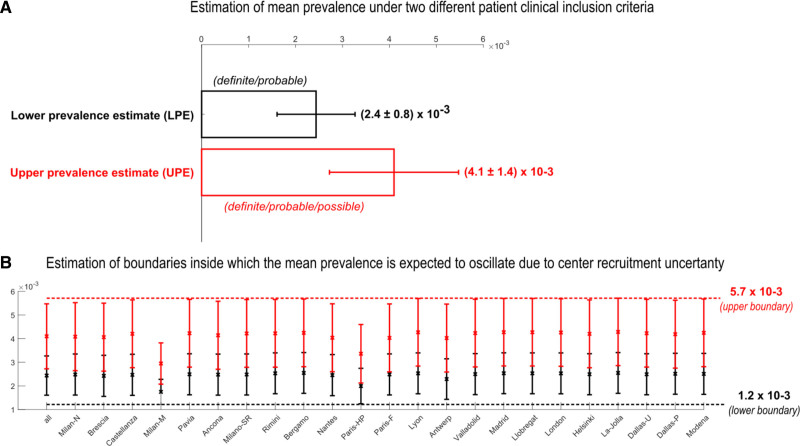
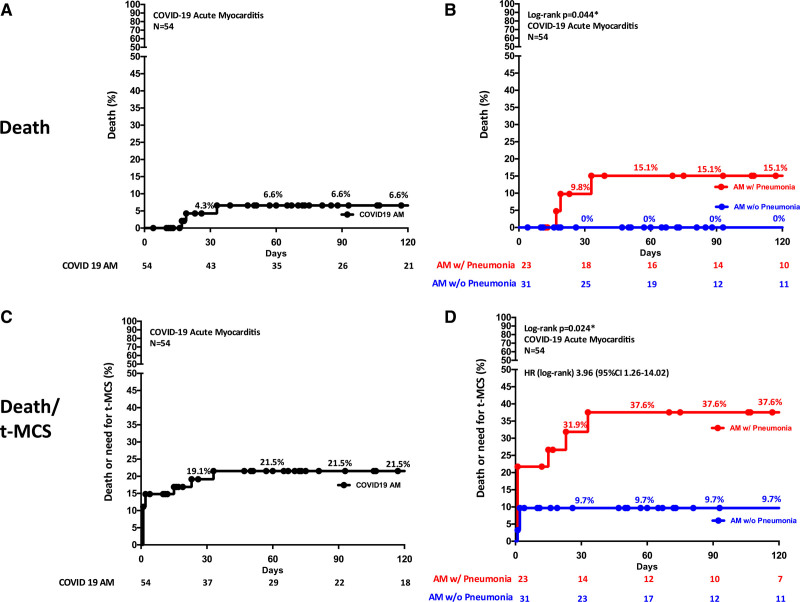
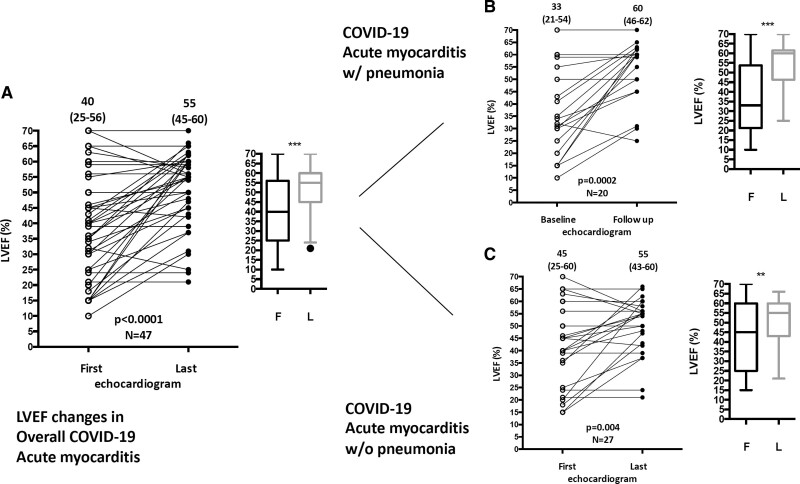
Results: AM prevalence among hospitalized patients with COVID-19 was 2.4 per 1000 hospitalizations considering definite/probable and 4.1 per 1000 considering also possible AM. The median age of definite/probable cases was 38 years, and 38.9% were female. On admission, chest pain and dyspnea were the most frequent symptoms (55.5% and 53.7%, respectively). Thirty-one cases (57.4%) occurred in the absence of COVID-19-associated pneumonia. Twenty-one (38.9%) had a fulminant presentation requiring inotropic support or temporary mechanical circulatory support. The composite of in-hospital mortality or temporary mechanical circulatory support occurred in 20.4%. At 120 days, estimated mortality was 6.6%, 15.1% in patients with associated pneumonia versus 0% in patients without pneumonia (P=0.044). During hospitalization, left ventricular ejection fraction, assessed by echocardiography, improved from a median of 40% on admission to 55% at discharge (n=47; P<0.0001) similarly in patients with or without pneumonia. Corticosteroids were frequently administered (55.5%).
Conclusions: AM occurrence is estimated between 2.4 and 4.1 out of 1000 patients hospitalized for COVID-19. The majority of AM occurs in the absence of pneumonia and is often complicated by hemodynamic instability. AM is a rare complication in patients hospitalized for COVID-19, with an outcome that differs on the basis of the presence of concomitant pneumonia.
Keywords: COVID-2019; MRI; SARS-CoV-2; cardiac; myocarditis; outcome.
Figures
References
-
- Berlin DA, Gulick RM, Martinez FJ. Severe Covid-19. N Engl J Med. 2020;383:2451–2460. doi: 10.1056/NEJMcp2009575 - PubMed
-
- Guo J, Huang Z, Lin L, Lv J. Coronavirus disease 2019 (COVID-19) and cardiovascular disease: a viewpoint on the potential influence of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers on onset and severity of severe acute respiratory syndrome coronavirus 2 infection. J Am Heart Assoc. 2020;9:e016219. doi: 10.1161/JAHA.120.016219 - PMC - PubMed
-
- Lala A, Johnson KW, Januzzi JL, Russak AJ, Paranjpe I, Richter F, Zhao S, Somani S, Van Vleck T, Vaid A, et al. ; Mount Sinai COVID Informatics Center. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol. 2020;76:533–546. doi: 10.1016/j.jacc.2020.06.007 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
