

Mortality rates among COVID-19 patients hospitalised during the first three waves of the epidemic in Milan, Italy: A prospective observational study
- PMID: 35404963
- PMCID: PMC9000097
- DOI: 10.1371/journal.pone.0263548
Mortality rates among COVID-19 patients hospitalised during the first three waves of the epidemic in Milan, Italy: A prospective observational study
Abstract
Introduction: This paper describes how mortality among hospitalised COVID-19 patients changed during the first three waves of the epidemic in Italy.
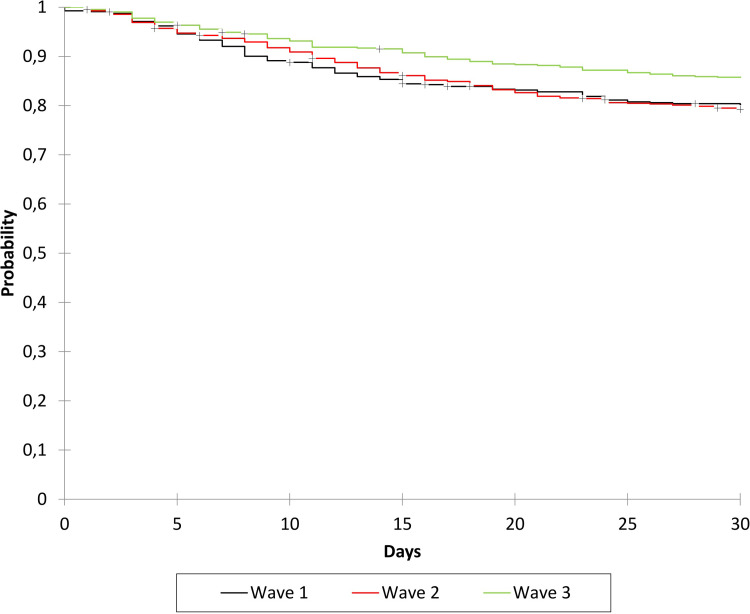
Methods: This prospective cohort study used the Kaplan-Meier method to analyse the time-dependent probability of death of all of the patients admitted to a COVID-19 referral centre in Milan, Italy, during the three consecutive periods of: 21 February-31 July 2020 (first wave, W1), 1 August 2020-31 January 2021 (second wave, W2), and 1 February-30 April 2021 (third wave, W3). Cox models were used to examine the association between death and the period of admission after adjusting for age, biological sex, the time from symptom onset to admission, disease severity upon admission, obesity, and the comorbidity burden.
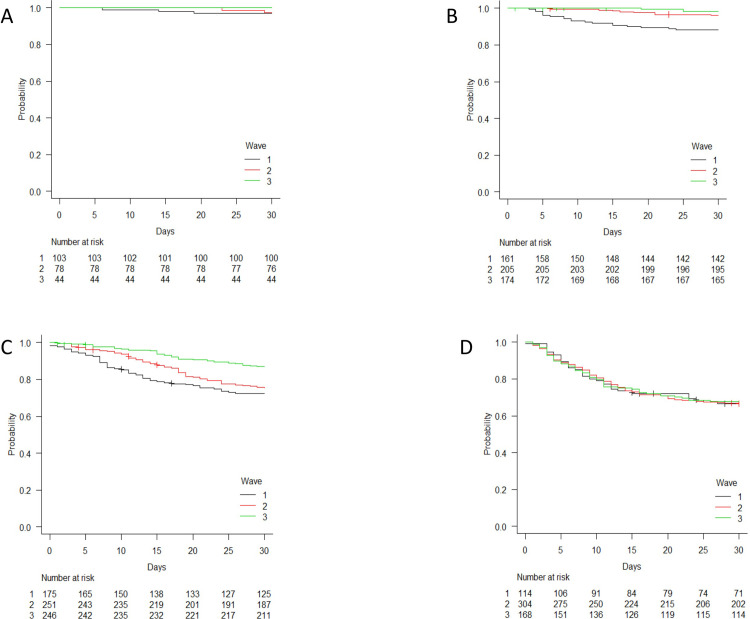
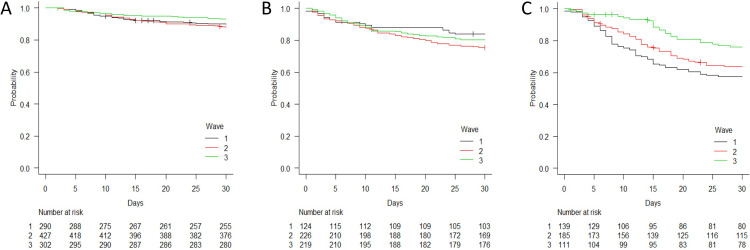
Results: Of the 2,023 COVID-19 patients admitted to our hospital during the study period, 553 (27.3%) were admitted during W1, 838 (41.5%) during W2, and 632 (31.2%) during W3. The crude mortality rate during W1, W2 and W3 was respectively 21.3%, 23.7% and 15.8%. After adjusting for potential confounders, hospitalisation during W2 or W3 was independently associated with a significantly lower risk of death than hospitalisation during W1 (adjusted hazard ratios [AHRs]: 0.75, 95% confidence interval [CI] 0.59-0.95, and 0.58, 95% CI 0.44-0.77). Among the patients aged >75 years, there was no significant difference in the probability of death during the three waves (AHRs during W2 and W3 vs W1: 0.93, 95% CI 0.65-1.33, and 0.88, 95% CI 0.59-1.32), whereas those presenting with critical disease during W2 and W3 were at significantly lower risk of dying than those admitted during W1 (AHRs 0.61, 95% CI 0.43-0.88, and 0.44, 95% CI 0.28-0.70).
Conclusions: Hospitalisation during W2 and W3 was associated with a reduced risk of COVID-19 death in comparison with W1, but there was no difference in survival probability in patients aged >75 years.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Weekly epidemiological update on COVID-19. https://covid19.who.int/ Accessed 18 January 2022.
-
- Menachemi N, Dixon BE, Wools-Kaloustian KK, Yiannoutsos CT, Halverson PK. How Many SARS-CoV-2-Infected People Require Hospitalization? Using Random Sample Testing to Better Inform Preparedness Efforts. J Public Health Manag Pract. 2021. May-Jun 01;27(3):246–250. doi: 10.1097/PHH.0000000000001331 . - DOI - PubMed
-
- Sudharsanan N, Didzun O, Bärnighausen T, Geldsetzer P. The Contribution of the Age Distribution of Cases to COVID-19 Case Fatality Across Countries: A Nine-Country Demographic Study. Ann Intern Med. 2020. Nov 3;173(9):714–720. doi: 10.7326/M20-2973 Epub 2020 Jul 22. ; PMCID: PMC7397549. - DOI - PMC - PubMed
-
- Dudel C, Riffe T, Acosta E, van Raalte A, Strozza C, Myrskylä M. Monitoring trends and differences in COVID-19 case-fatality rates using decomposition methods: Contributions of age structure and age-specific fatality. PLoS One. 2020. Sep 10;15(9):e0238904. doi: 10.1371/journal.pone.0238904 ; PMCID: PMC7482960. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
