

Discontinuing vs continuing ACEIs and ARBs in hospitalized patients with COVID-19 according to disease severity: Insights from the BRACE CORONA trial
- PMID: 35405099
- PMCID: PMC8993458
- DOI: 10.1016/j.ahj.2022.04.001
Discontinuing vs continuing ACEIs and ARBs in hospitalized patients with COVID-19 according to disease severity: Insights from the BRACE CORONA trial
Abstract
Background: We explored the effect of discontinuing versus continuing angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) on clinical outcomes in patients with COVID-19 according to baseline disease severity.
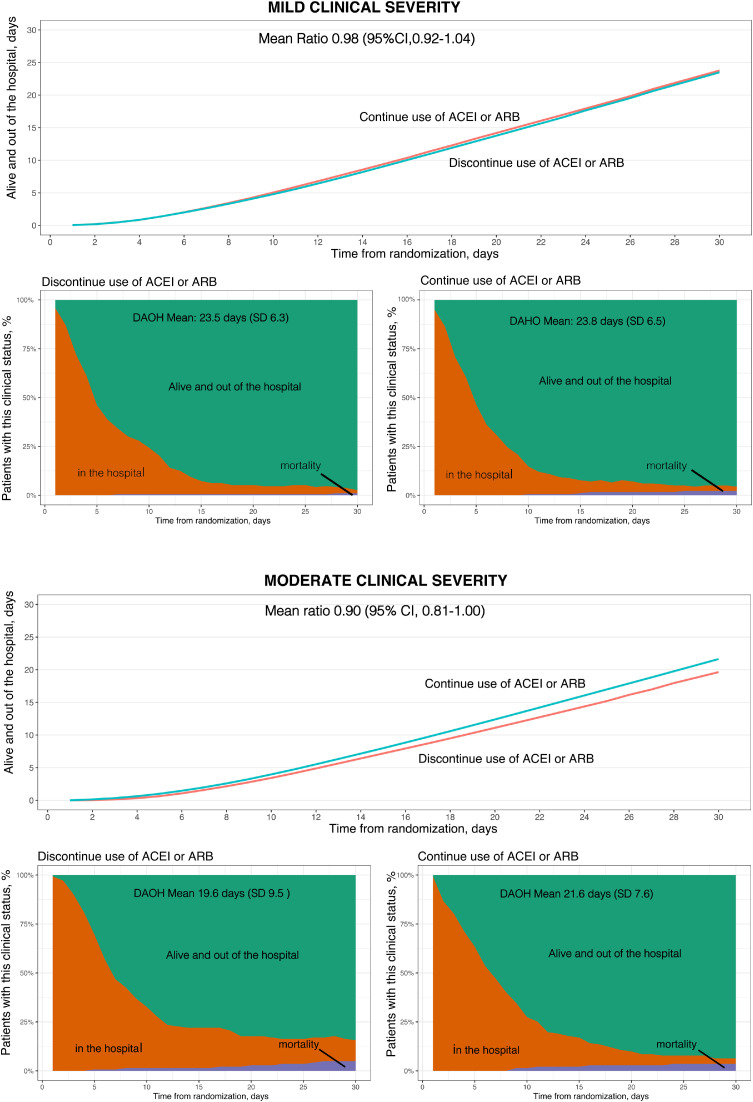
Methods: We randomized 659 patients with a confirmed diagnosis of COVID-19 and classified them as having mild or moderate COVID-19 disease severity at hospital presentation using blood oxygen saturation and lung imaging. The primary outcome was the mean ratio of number of days alive and out of the hospital at 30 days according to disease severity.
Results: At presentation, 376 patients (57.1%) had mild and 283 (42.9%) had moderate COVID-19. In patients with mild disease, there was no significant difference in the number of days alive and out of the hospital between ACEI/ARB discontinuation (mean 23.5 [SD 6.3] days) and continuation (mean 23.8 [SD 6.5] days), with a mean ratio of 0.98 (95% CI 0.92-1.04). However, in patients with moderate disease, there were fewer days alive and out of the hospital with ACEI/ARB discontinuation (mean 19.6 [SD 9.5] days) than continuation (mean 21.6 [SD 7.6] days), with a mean ratio of 0.90 (95% CI 0.81-1.00; P-interaction = .01). The impact of discontinuing versus continuing ACEIs/ARBs on days alive and out of hospital through 30 days differed according to baseline COVID-19 disease severity.
Conclusions: Unlike patients with mild disease, patients with moderate disease who continued ACEIs/ARBs had more days alive and out of hospital through 30 days than those who discontinued ACEIs/ARBs. This suggests that ACEIs/ARBs should be continued for patients with moderate COVID-19 disease severity.
Clinical trial registration: ClinicalTrials.gov (NCT04364893).
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures

References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239–1242. - PubMed
