

Persistence of immunogenicity after seven COVID-19 vaccines given as third dose boosters following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK: Three month analyses of the COV-BOOST trial
- PMID: 35405168
- PMCID: PMC8993491
- DOI: 10.1016/j.jinf.2022.04.018
Persistence of immunogenicity after seven COVID-19 vaccines given as third dose boosters following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK: Three month analyses of the COV-BOOST trial
Erratum in
-
Corrigendum to "Persistence of immunogenicity after seven COVID-19 vaccines given as third dose boosters following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK: Three month analyses of the COV-BOOST trial" [J Infect 84(6) (2022) 795-813, 5511].J Infect. 2023 May;86(5):540-541. doi: 10.1016/j.jinf.2023.03.025. Epub 2023 Apr 12. J Infect. 2023. PMID: 37055303 Free PMC article. No abstract available.
Abstract
Objectives: To evaluate the persistence of immunogenicity three months after third dose boosters.
Methods: COV-BOOST is a multicentre, randomised, controlled, phase 2 trial of seven COVID-19 vaccines used as a third booster dose. The analysis was conducted using all randomised participants who were SARS-CoV-2 naïve during the study.
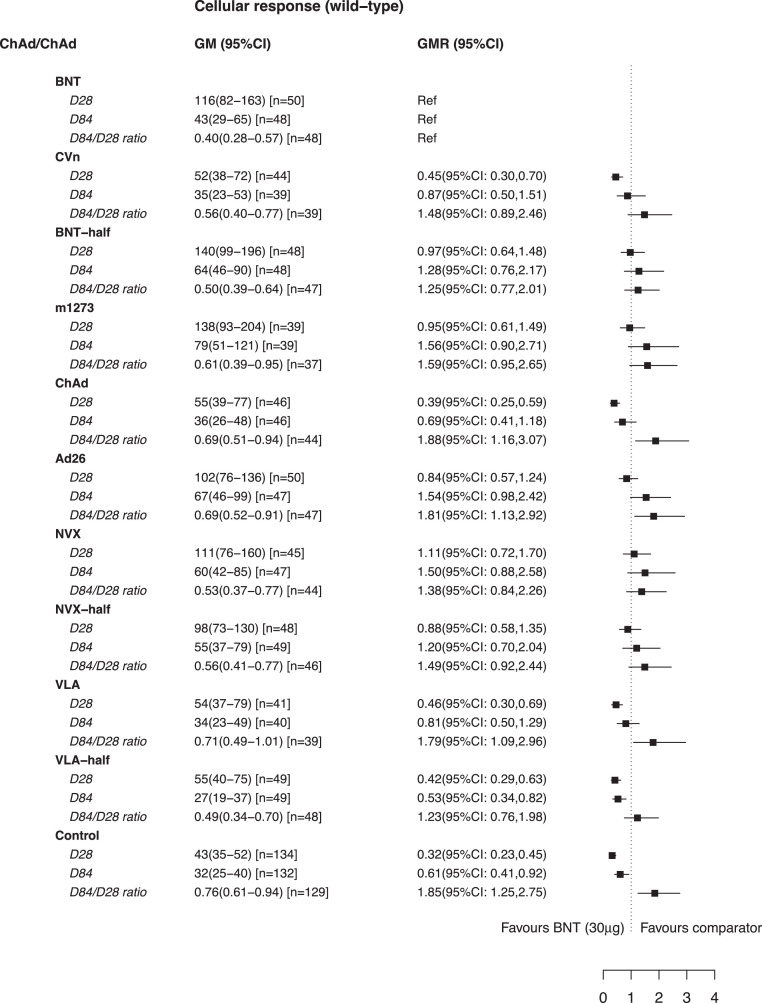
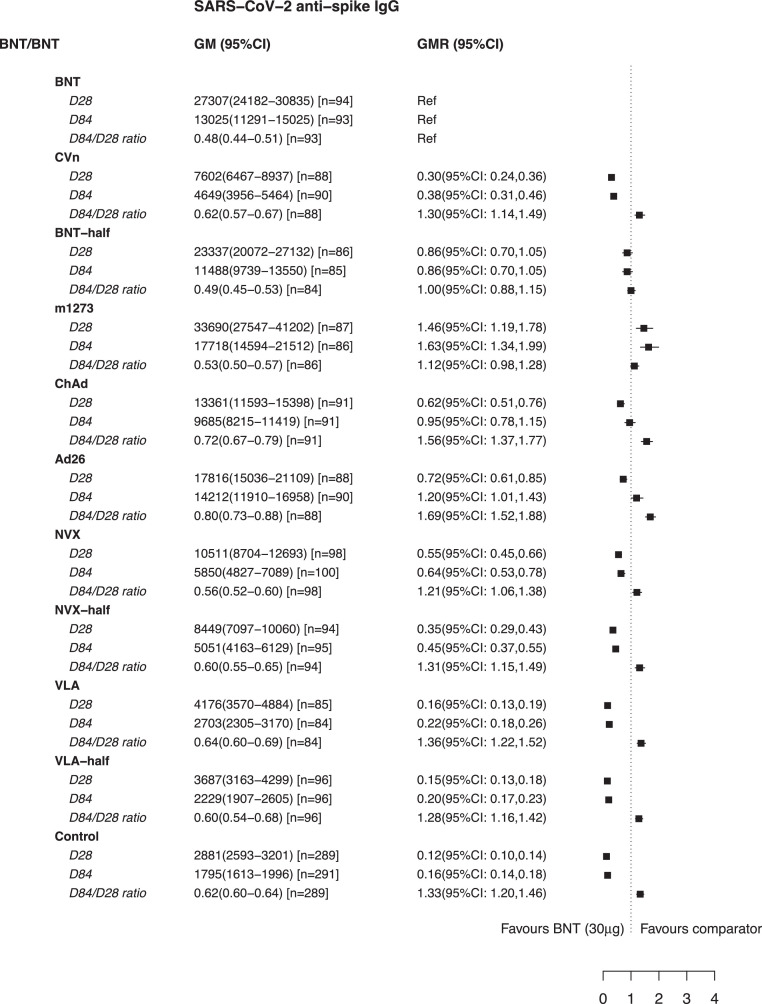
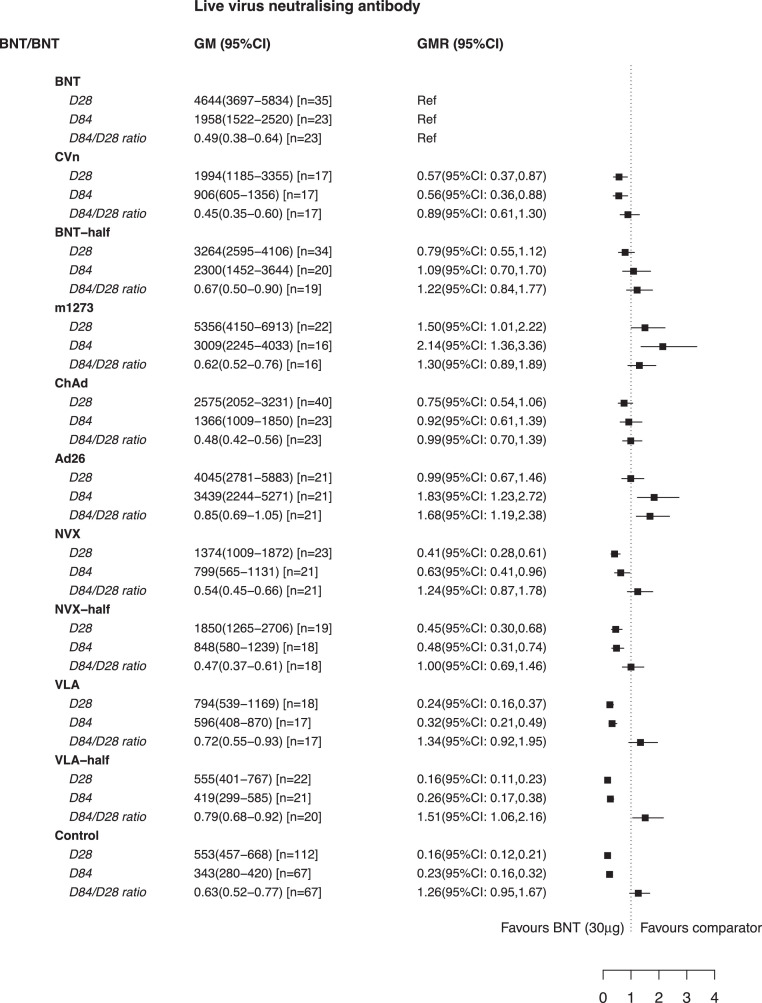
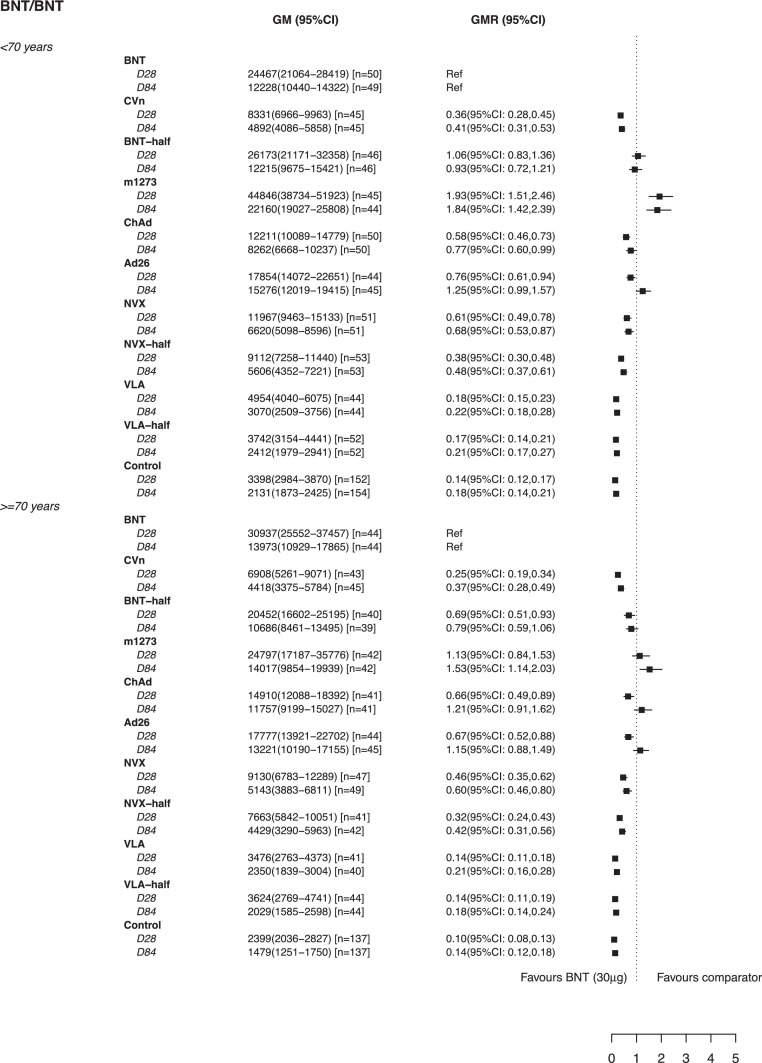
Results: Amongst the 2883 participants randomised, there were 2422 SARS-CoV-2 naïve participants until D84 visit included in the analysis with median age of 70 (IQR: 30-94) years. In the participants who had two initial doses of ChAdOx1 nCov-19 (Oxford-AstraZeneca; hereafter referred to as ChAd), schedules using mRNA vaccines as third dose have the highest anti-spike IgG at D84 (e.g. geometric mean concentration of 8674 ELU/ml (95% CI: 7461-10,085) following ChAd/ChAd/BNT162b2 (Pfizer-BioNtech, hearafter referred to as BNT)). However, in people who had two initial doses of BNT there was no significant difference at D84 in people given ChAd versus BNT (geometric mean ratio (GMR) of 0.95 (95%CI: 0.78, 1.15). Also, people given Ad26.COV2.S (Janssen; hereafter referred to as Ad26) as a third dose had significantly higher anti-spike IgG at D84 than BNT (GMR of 1.20, 95%CI: 1.01,1.43). Responses at D84 between people who received BNT (15 μg) or BNT (30 μg) after ChAd/ChAd or BNT/BNT were similar, with anti-spike IgG GMRs of half-BNT (15 μg) versus BNT (30 μg) ranging between 0.74-0.86. The decay rate of cellular responses were similar between all the vaccine schedules and doses.
Conclusions: 84 days after a third dose of COVID-19 vaccine the decay rates of humoral response were different between vaccines. Adenoviral vector vaccine anti-spike IgG concentrations at D84 following BNT/BNT initial doses were similar to or even higher than for a three dose (BNT/BNT/BNT) schedule. Half dose BNT immune responses were similar to full dose responses. While high antibody tires are desirable in situations of high transmission of new variants of concern, the maintenance of immune responses that confer long-lasting protection against severe disease or death is also of critical importance. Policymakers may also consider adenoviral vector, fractional dose of mRNA, or other non-mRNA vaccines as third doses.
Keywords: COVID-19 vaccine; Fractional dose; Heterologous boost; Homologous boost; Immunogenicity; Persistence; Third dose.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest KC acts on behalf of University Hospital Southampton as an investigator on studies funded or sponsored by vaccine manufacturers including AstraZeneca, GlaxoSmithKline, Janssen, Medimmune, Merck, Pfizer, Sanofi and Valneva. She receives no personal financial payment for this work. SNF acts on behalf of University Hospital Southampton NHS Foundation Trust as an Investigator and/or providing consultative advice on clinical trials and studies of COVID-19 and other vaccines funded or sponsored by vaccine manufacturers including Janssen, Pfizer, AstraZeneca, GlaxoSmithKline, Novavax, Seqirus, Sanofi, Medimmune, Merck and Valneva vaccines and antimicrobials. He receives no personal financial payment for this work. ALG is named as an inventor on a patent covering use of a particular promoter construct that is often used in ChAdOx1-vectored vaccines and is incorporated in the ChAdOx1 nCoV-19 vaccine. ALG may benefit from royalty income paid to the University of Oxford from sales of this vaccine by AstraZeneca and its sublicensees under the University's revenue sharing policy. JH has received payments for presentations for AstraZeneca, Boehringer Ingelheim, Chiesi, Ciple & Teva. VL acts on behalf of University College London Hospitals NHS Foundation Trust as an Investigator on clinical trials of COVID-19 vaccines funded or sponsored by vaccine manufacturers including Pfizer, AstraZeneca and Valneva. He receives no personal financial payment for this work. PM acts on behalf of University Hospital Southampton NHS Foundation Trust and The Adam Practice as an investigator on studies funded or sponsored by vaccine manufacturers including AstraZeneca, GlaxoSmithKline, Novavax, Medicago and Sanofi. He received no personal financial payment for this work. JSN-V-T is seconded to the Department of Health and Social Care, England until 31st March 2022. MR has provided post marketing surveillance reports on vaccines for Pfizer and GSK for which a cost recover charge is made. MDS acts on behalf of the University of Oxford as an investigator on studies funded or sponsored by vaccine manufacturers including AstraZeneca, GlaxoSmithKline, Pfizer, Novavax. Janssen, Medimmune and MCM vaccines. He received no personal financial payment for this work.
Figures












References
-
- OurWorldinData. COVID-19 vaccine booster doses administered per 100 people. 2021. Available from: https://ourworldindata.org/grapher/covid-vaccine-booster-doses-per-capita.
-
- Munro A.P.S., Janani L., Cornelius V., Aley P.K., Babbage G., Baxter D., et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): a blinded, multicentre, randomised, controlled, phase 2 trial. Lancet. 2021 - PMC - PubMed
-
- Lyngse F.P., Kirkeby C.T., Denwood M., Christiansen L.E., Mølbak K., Møller C.H., et al. Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: evidence from Danish Households. medRxiv. 2022: 2022.01.28. 22270044.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
