

The Role of Simultaneous Integrated Boost in Locally Advanced Rectal Cancer Patients with Positive Lateral Pelvic Lymph Nodes
- PMID: 35406415
- PMCID: PMC8996944
- DOI: 10.3390/cancers14071643
The Role of Simultaneous Integrated Boost in Locally Advanced Rectal Cancer Patients with Positive Lateral Pelvic Lymph Nodes
Abstract
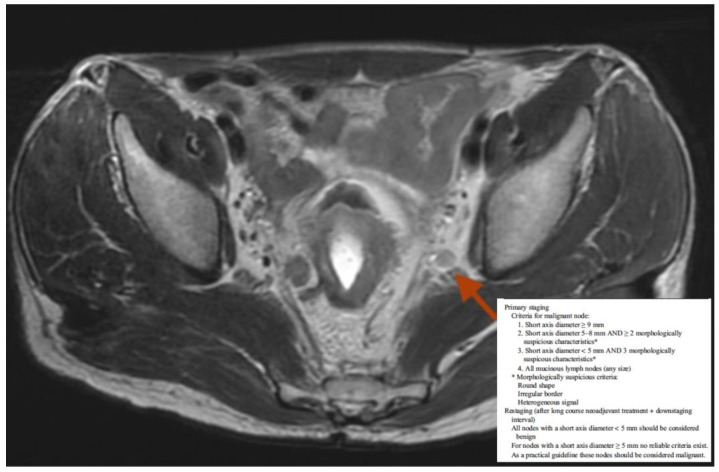
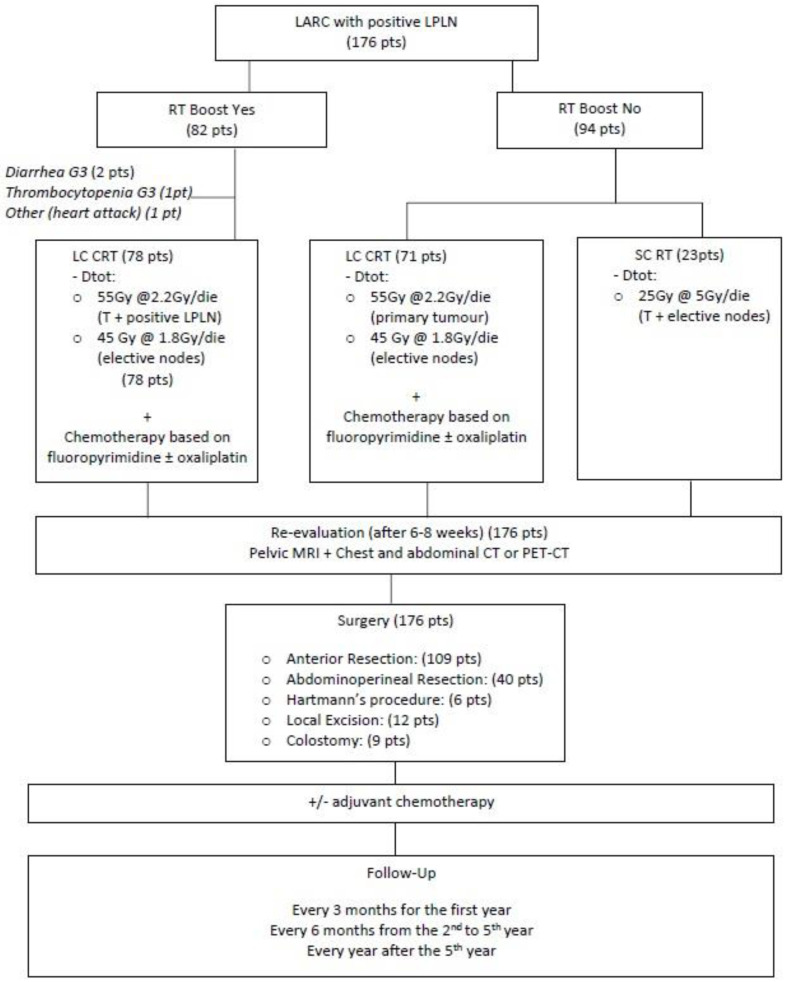
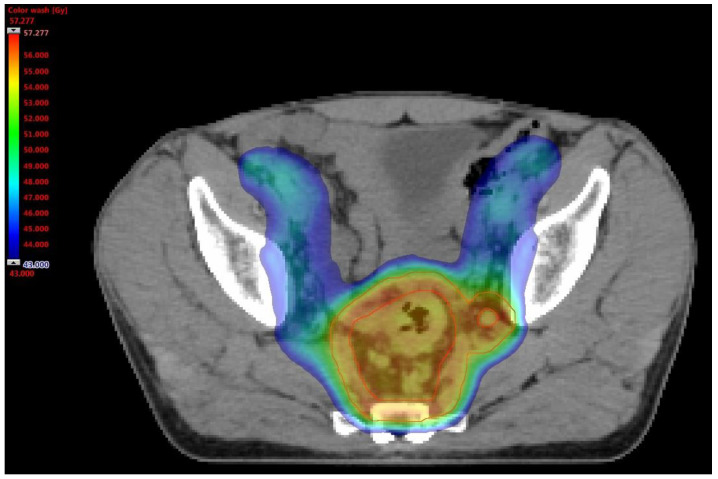
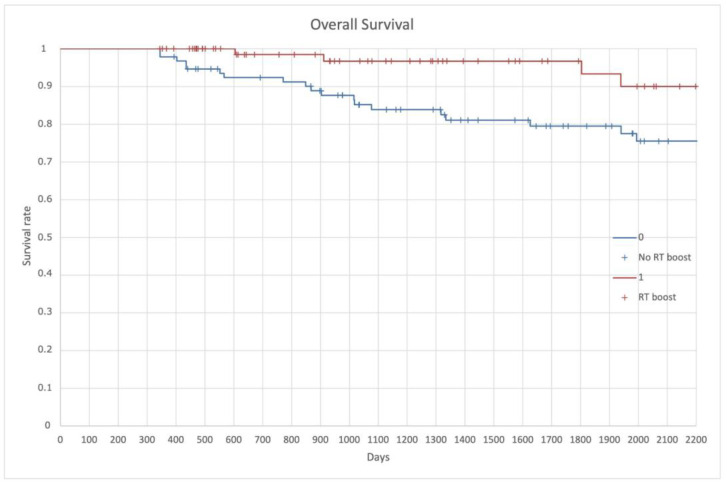
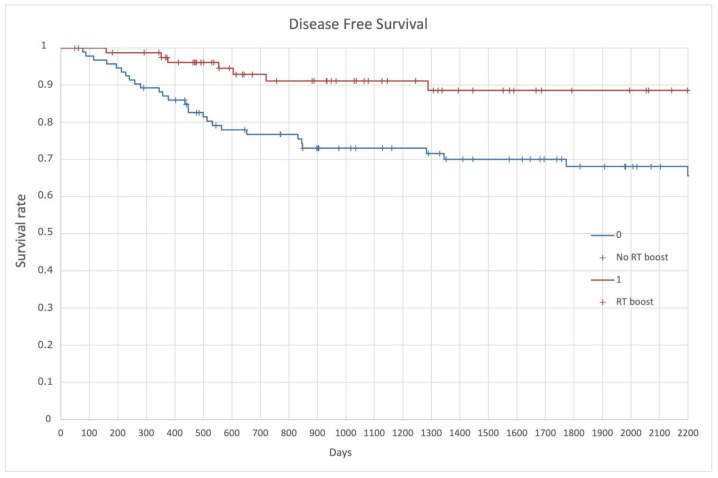
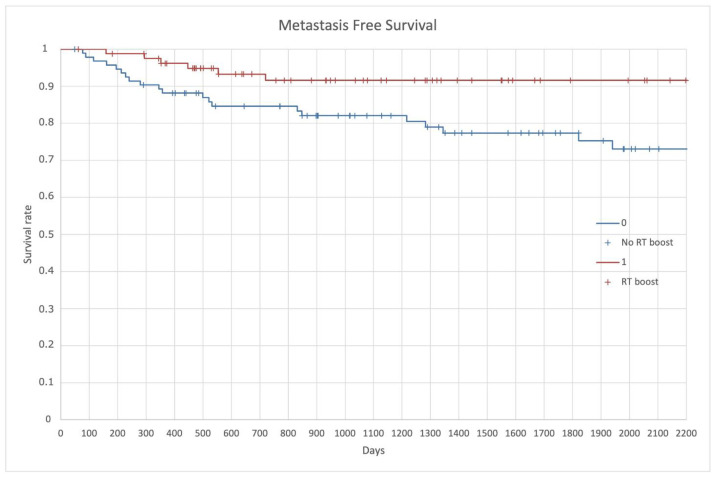
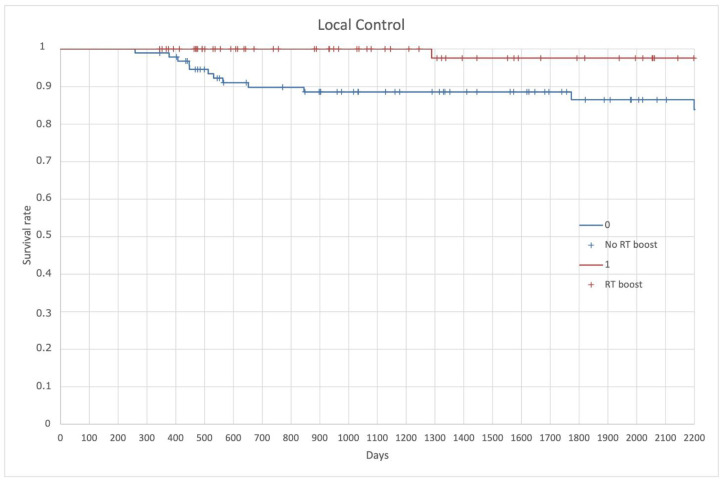
Aims: Between 11 to 14% of patients with locally advanced rectal cancer (LARC) have positive lateral pelvic lymph nodes (LPLN) at diagnosis, related to a worse prognosis with a 5-year survival rate between 30 to 40%. The best treatment choice for this group of patients is still a challenge. The optimal radiotherapy (RT) dose for LPLN patients has been investigated. Methods: We retrospectively collected data from LARC patients with LPLN at the primary staging MRI, treated in our center from March 2003 to December 2020. Patients underwent a neoadjuvant concomitant chemo-radiotherapy (CRT) treatment on the primary tumor (T), mesorectum, and pelvic nodes, associated with a fluoride-based chemotherapy. The total reached dose was 45 Gy at 1.8 Gy/fr on the elective sites and 55 Gy at 2.2 Gy/fr on the disease and mesorectum. Patients were divided in two groups based on whether they received a simultaneous integrated RT boost on the LPLN or not. Overall Survival (OS), Disease Free Survival (DFS), Metastasis Free Survival (MFS), and Local Control (LC) were evaluated in the whole group and then compared between the two groups. Results: A total of 176 patients were evaluated: 82 were included in the RT boost group and 94 in the non-RT boost group. The median follow-up period was 57.8 months. All the clinical endpoint (OS, DFS, MFS, LC), resulted were affected by the simultaneous integrated boost on LPLN with a survival rate of 84.7%, 79.5%, 84.1%, and 92%, respectively, in the entire population. From the comparison of the two groups, there was a statistical significance towards the RT boost group with a p < 0.006, 0.030, 0.042, 0.026, respectively. Conclusions: Concomitant radiotherapy boost on positive LPLN has shown to be beneficial on the survival outcomes (OS, DFS, MFR, and LC) in patients with LARC and LPLN. This analysis demonstrates that a higher dose of radiotherapy on positive pelvic lymph nodes led not only to a higher local control but also to a better survival rate. These results, if validated by future prospective studies, can bring a valid alternative to the surgery dissection without the important side effects and permanent disabilities observed during the years.
Keywords: chemoradiotherapy; lateral pelvic positive nodes; locally advanced rectal cancer; radiotherapy; simultaneous integrated boost.
Conflict of interest statement
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Shiratori H., Kawai K., Hata K., Tanaka T., Nishikawa T., Sasaki K., Kaneko M., Murono K., Emoto S., Morikawa T., et al. Correlations between the Recurrence Patterns and Sizes of Lateral Pelvic Lymph Nodes before and after Chemoradiotherapy in Patients with Lower Rectal Cancer. Oncology. 2019;96:33–43. doi: 10.1159/000492493. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
