

Extranodal Marginal Zone Lymphoma: Pathogenesis, Diagnosis and Treatment
- PMID: 35406516
- PMCID: PMC8997163
- DOI: 10.3390/cancers14071742
Extranodal Marginal Zone Lymphoma: Pathogenesis, Diagnosis and Treatment
Abstract
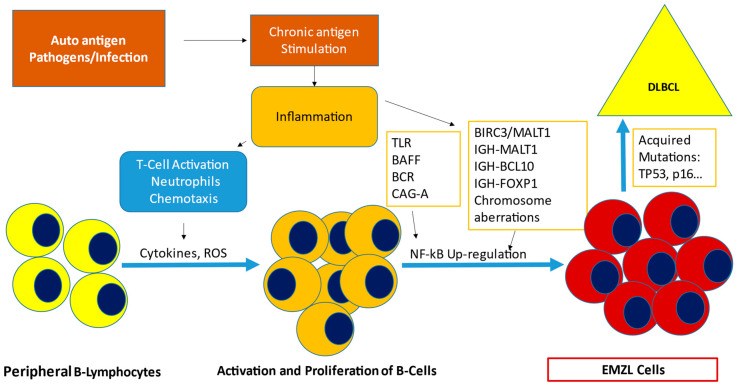
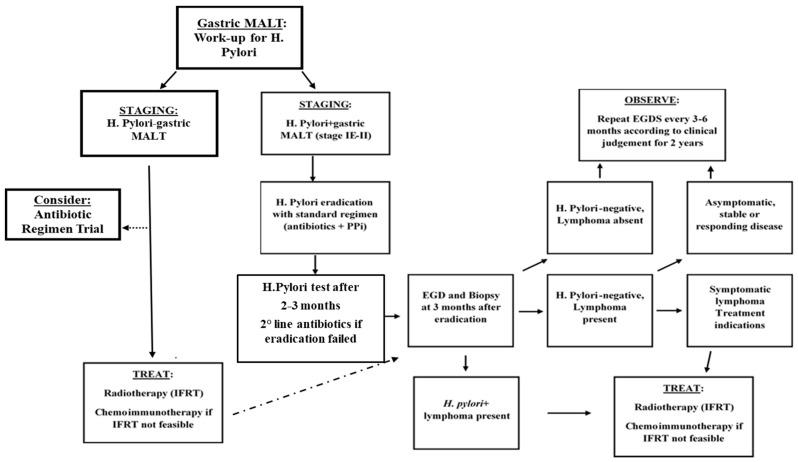
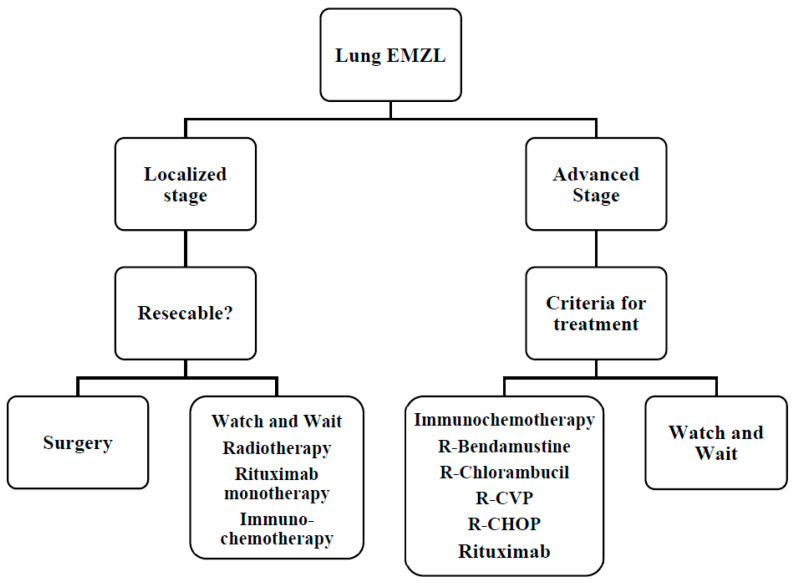
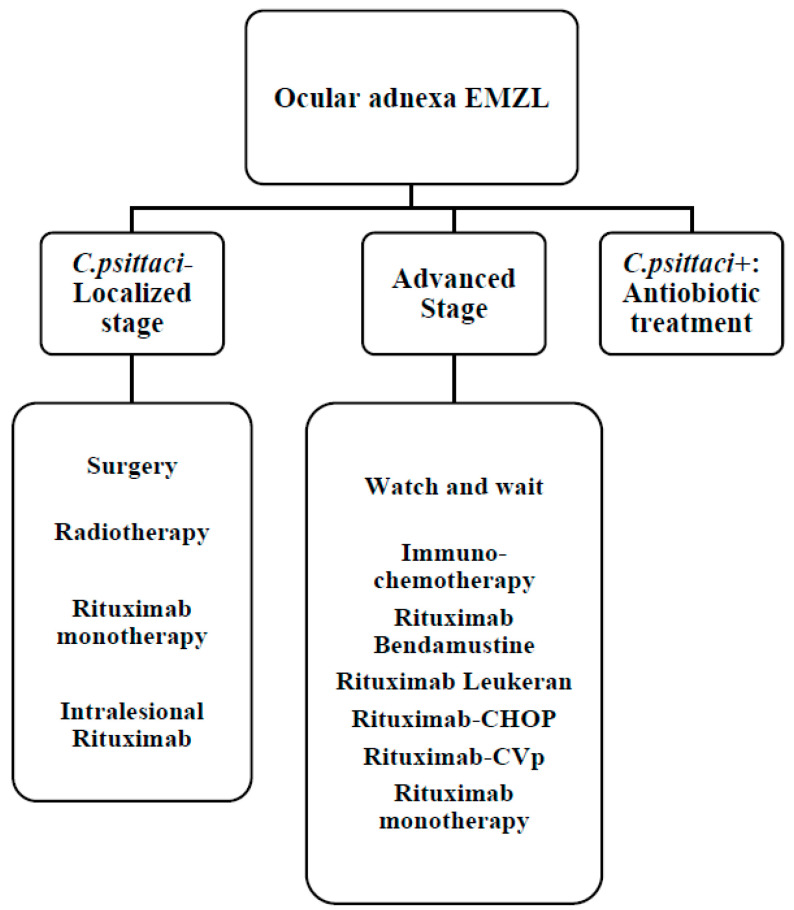
Extranodal Marginal Zone Lymphoma (EMZL lymphoma) is an indolent B-cell lymphoma with a median age at diagnosis of about 60 years. It accounts for 7-8% of all B-cell lymphomas. It can occur in various extranodal sites, including stomach, lung, ocular adnexa, and skin; furthermore, the disseminated disease can be found in 25-50% of cases. Several infectious agents, such as Helicobacter pylori (H. Pylori) in the case of gastric Mucosa Associated Lymphoid Tissue (MALT) Lymphoma, can drive the pathogenesis of this cancer, through the autoantigenic stimulation of T cells, but there may also be other factors participating such autoimmune diseases. Initial staging should include total body computed tomography, bone marrow aspirate, and endoscopic investigation if indicated. Fluorescence in situ hybridization (FISH), should be performed to detect the presence of specific chromosomal translocations involving the MALT1 and BCL10 genes, which leads to the activation of the NF-κB signaling pathway. Depending on the location and dissemination of the disease, different therapeutic choices may include targeted therapy against the etiopathogenetic agent, radiotherapy, immunochemotherapy, and biological drugs. The purpose of this review is to illustrate the complex biology and the diagnosis of this disease and to better define new treatment strategies.
Keywords: BALT; MALT; OAL; diagnosis; immunotherapy; marginal zone lymphoma; non-Hodgkin lymphoma; prognosis; targeted-therapy; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Swerdlow S.H., Campo E., Pileri S.A., Harris N.L., Stein H., Siebert R., Advani R., Ghielmini M., Salles G.A., Zelenetz A.D., et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375–2390. doi: 10.1182/blood-2016-01-643569. - DOI - PMC - PubMed
-
- Smedby K.E., Vajdic C.M., Falster M., Engels E.A., Martínez-Maza O., Turner J., Hjalgrim H., Vineis P., Costantini A.S., Bracci P.M., et al. Autoimmune disorders and risk of non-Hodgkin lymphoma subtypes: A pooled analysis within the InterLymph Consortium. Blood. 2008;111:4029–4038. doi: 10.1182/blood-2007-10-119974. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
