

Utilization of Immunotherapy for the Treatment of Hepatocellular Carcinoma in the Peri-Transplant Setting: Transplant Oncology View
- PMID: 35406533
- PMCID: PMC8997123
- DOI: 10.3390/cancers14071760
Utilization of Immunotherapy for the Treatment of Hepatocellular Carcinoma in the Peri-Transplant Setting: Transplant Oncology View
Abstract
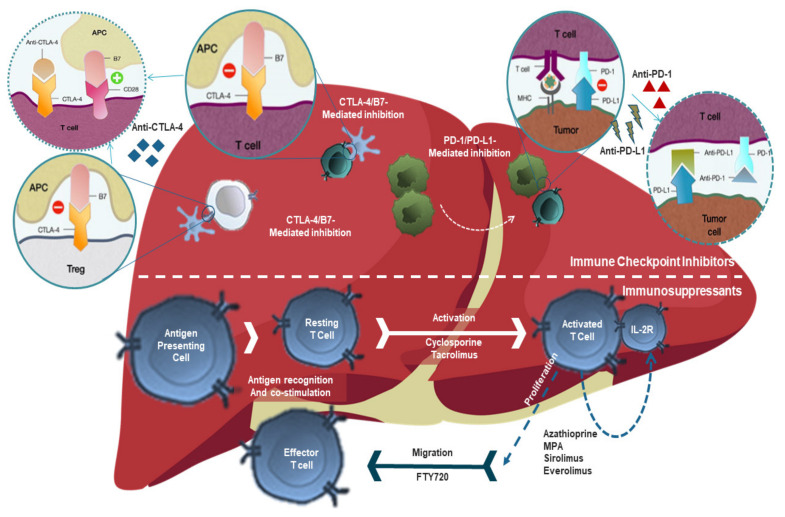
Hepatocellular carcinoma (HCC) represents the second most common cause of cancer-related deaths and accounts for over eighty percent of primary liver cancers worldwide. Surgical resection and radiofrequency ablation in small tumors are included in the treatment options for HCC patients with good liver function profiles. According to the Milan Criteria, only a small portion of HCC patients are eligible for liver transplantation due to advanced-stage disease and large tumor size preventing/delaying organ allocation. Recently, the use of anti-programmed cell death protein 1 and programmed cell death ligand 1 (PD-1 and PD-L1) checkpoint inhibitors in the treatment of cancers have evolved rapidly and these therapies have been approved for the treatment of HCC. Immune checkpoint inhibitors have resulted in good clinical outcomes in pre-and post-transplant HCC patients, although, some reports showed that certain recipients may face rejection and graft loss. In this review, we aim to illustrate and summarize the utilization of immune checkpoint inhibitor therapies in pre-and post-liver transplants for HCC patients and discuss the assessment of immune checkpoint inhibitor regulators that might determine liver transplant outcomes.
Keywords: CTLA-4 inhibitors; PD-1 inhibitors; allograft rejection; hepatocellular carcinoma; immune checkpoint inhibitors; immunotherapy; liver transplantation; transplant oncology.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Abdelrahim M., Victor D., Esmail A., Kodali S., Graviss E.A., Nguyen D.T., Moore L.W., Saharia A., McMillan R., Fong J.N., et al. Transarterial Chemoembolization (TACE) plus sorafenib compared to TACE alone in transplant recipients with hepatocellular carcinoma: An institution experience. Cancers. 2022;14:650. doi: 10.3390/cancers14030650. - DOI - PMC - PubMed
-
- Abou-Alfa G.K., Meyer T., Cheng A.-L., El-Khoueiry A.B., Rimassa L., Ryoo B.-Y., Cicin I., Merle P., Park J.-W., Blanc J.-F., et al. Cabozantinib (C) versus placebo (P) in patients (pts) with advanced hepatocellular carcinoma (HCC) who have received prior sorafenib: Results from the randomized phase III CELESTIAL trial. J. Clin. Oncol. 2018;36:207. doi: 10.1200/JCO.2018.36.4_suppl.207. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
