

Ocular Complications of Giant Cell Arteritis: An Acute Therapeutic Emergency
- PMID: 35407604
- PMCID: PMC8999894
- DOI: 10.3390/jcm11071997
Ocular Complications of Giant Cell Arteritis: An Acute Therapeutic Emergency
Abstract
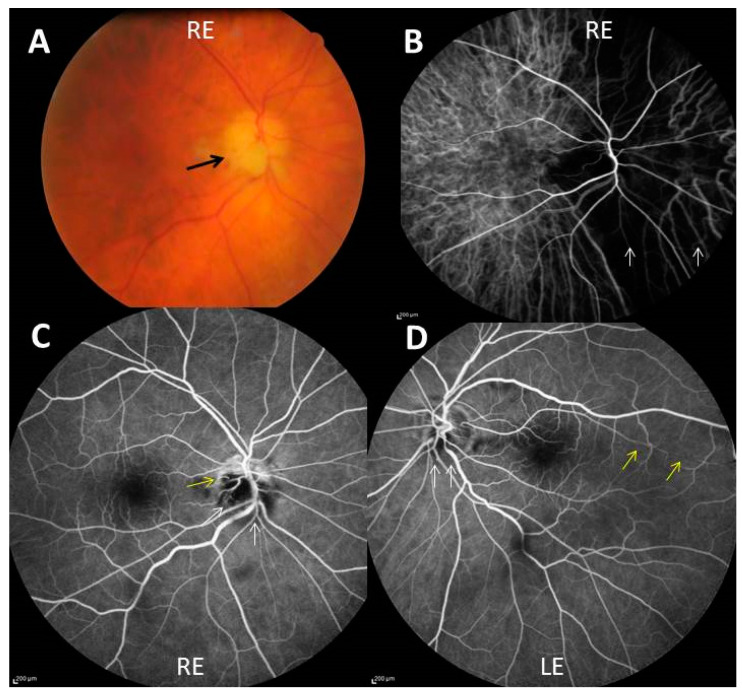
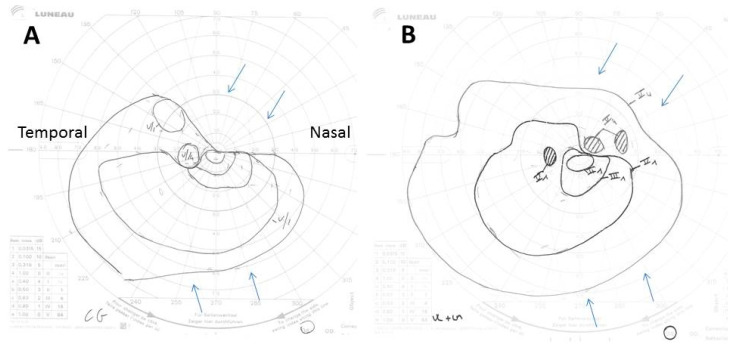
The risk of blindness, due to acute ischemic ocular events, is the most feared complication of giant cell arteritis (GCA) since the middle of the 20th century. A decrease of its rate has occurred after the advent of corticoid therapy for this vasculitis, but it seems to have stabilized since then. Early diagnosis and treatment of GCA is key to reducing its ocular morbidity. However, it is not uncommon for ophthalmological manifestations to inaugurate the disease, and the biological inflammatory reaction may be mild, making its diagnosis more challenging. In recent years, vascular imaging has opened up new possibilities for the rapid diagnosis of GCA, and ultrasound has taken a central place in fast-track diagnostic processes. Corticosteroid therapy remains the cornerstone of treatment and must begin immediately in patients with visual symptoms and suspicion of GCA. In that situation, the administration route of corticotherapy, intravenous or oral, is less important than its speed of delivery, any hour of delay worsening the prognosis.
Keywords: diagnosis; giant cell arteritis; ophthalmologic manifestations; treatment.
Conflict of interest statement
Emmanuel HERON: Roche-Chugai (remuneration for symposium and as consultant), Abbvie (invitation in congress).
Figures
References
-
- Horton B.T., Magath T.B., Brown G.E. An undescribed form of arteritis of the temporal vessels. Proc. Staff Meet. Mayo Clinic. 1932;7:700–701.
-
- Chasnoff J., Vorzimer J.J. Temporal arteritis: A local manifestation of a systemic disease. Ann. Intern. Med. 1944;20:327. doi: 10.7326/0003-4819-20-2-327. - DOI
-
- Gilmour J.R. Giant-cell chronic arteritis. J. Pathol. Bacteriol. 1941;53:263–277. doi: 10.1002/path.1700530210. - DOI
Publication types
LinkOut - more resources
Full Text Sources
