

Dislocation Arthropathy of the Shoulder
- PMID: 35407627
- PMCID: PMC8999818
- DOI: 10.3390/jcm11072019
Dislocation Arthropathy of the Shoulder
Abstract
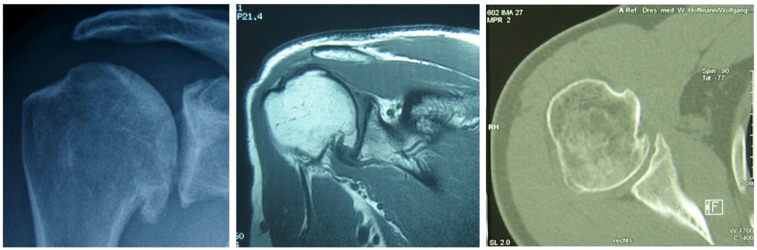
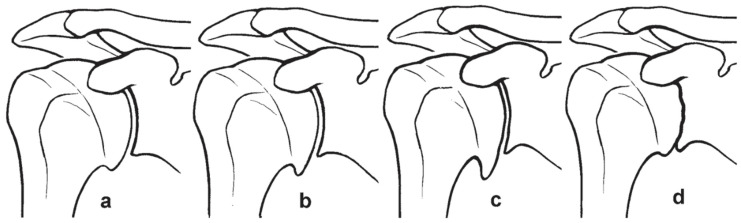
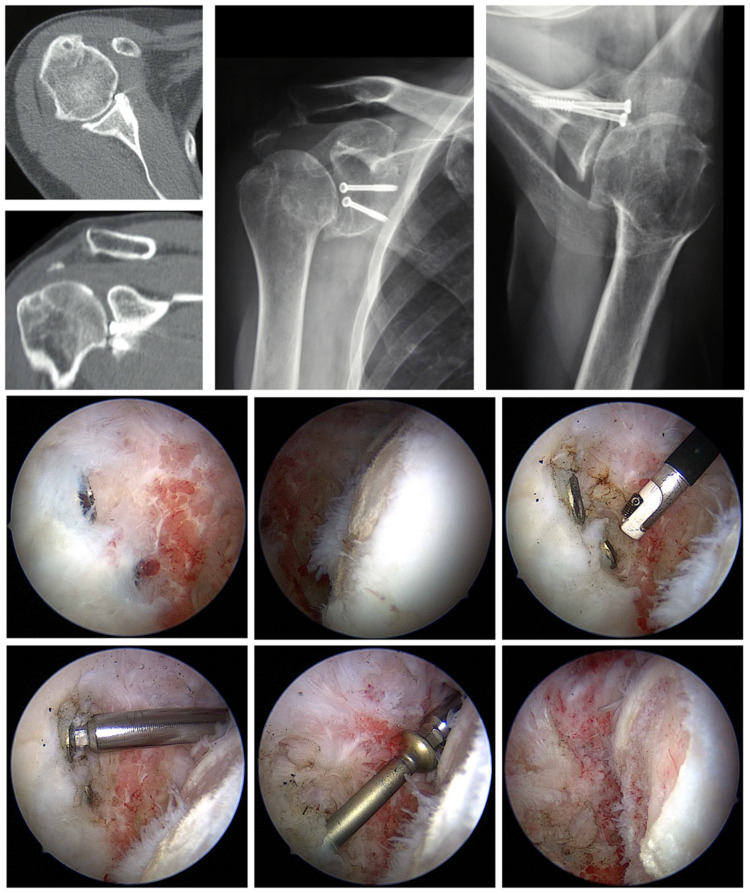
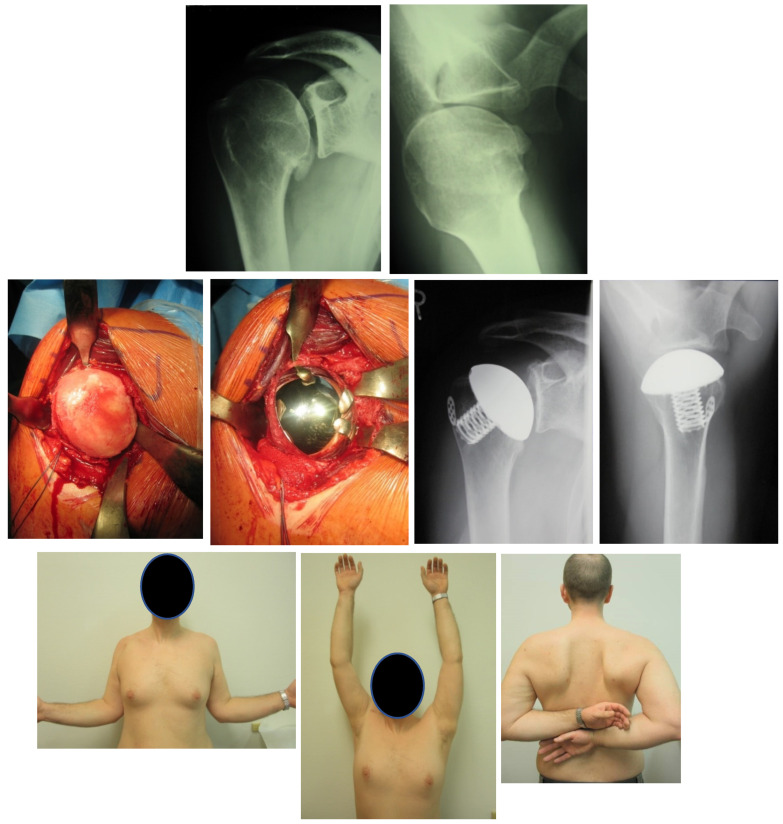
Glenohumeral osteoarthrosis (OA) may develop after primary, recurrent shoulder dislocation or instability surgery. The incidence is reported from 12 to 62%, depending on different risk factors. The risk of severe OA of the shoulder following dislocation is 10 to 20 times greater than the average population. Risk factors include the patient's age at the first episode of instability or instability surgery, bony lesions, and rotator cuff tears. For mild stages of OA, arthroscopic removal of intraarticular material, arthroscopic debridement, or arthroscopic arthrolysis of an internal rotation contracture might be sufficient. For severe stages, mobilization of the internal rotation contracture and arthroplasty is indicated. With an intact rotator cuff and without a bone graft, results for anatomical shoulder arthroplasty are comparable to those following primary OA. With a bone graft at the glenoidal side, the risk for implant loosening is ten times greater. For the functional outcome, the quality of the rotator cuff is more predictive than the type of the previous surgery or the preoperative external rotation contracture. Reverse shoulder arthroplasty could be justified due to the higher rate of complications and revisions of non-constrained anatomic shoulder arthroplasties reported. Satisfactory clinical and radiological results have been published with mid to long term data now available.
Keywords: arthroplasty; dislocation arthropathy; glenohumeral osteoarthrosis; shoulder dislocation; shoulder instability.
Conflict of interest statement
Ulrich H. Brunner and Markus Scheibel are consultant for Stryker.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
