

Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial
- PMID: 35407655
- PMCID: PMC8999405
- DOI: 10.3390/jcm11072047
Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial
Abstract
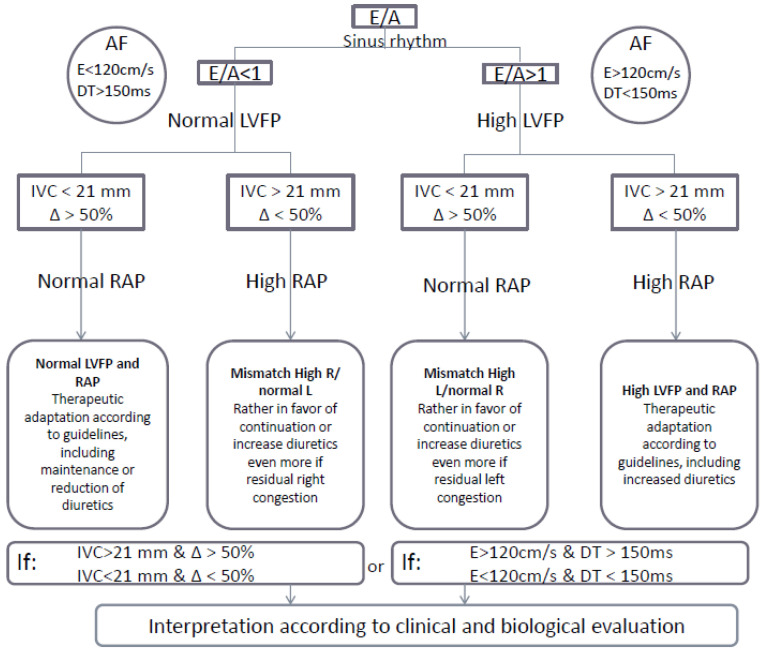
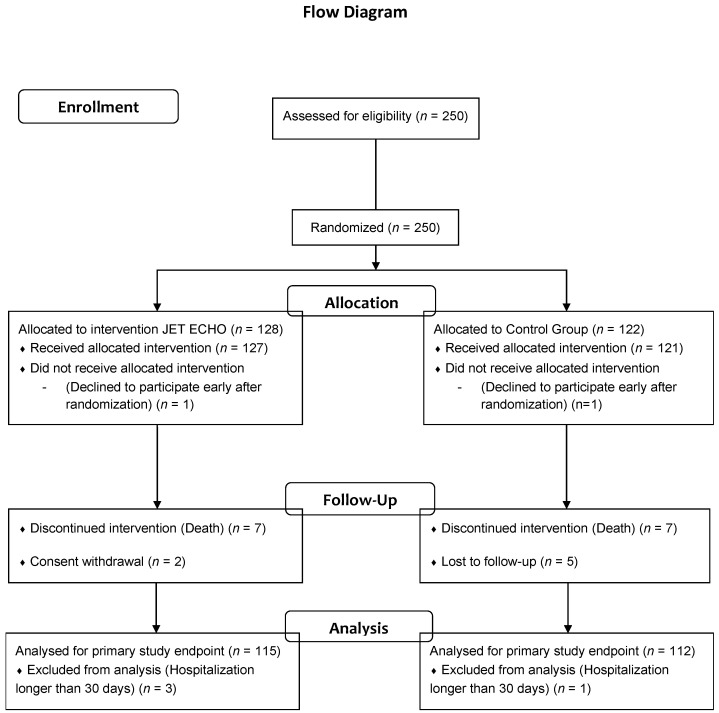
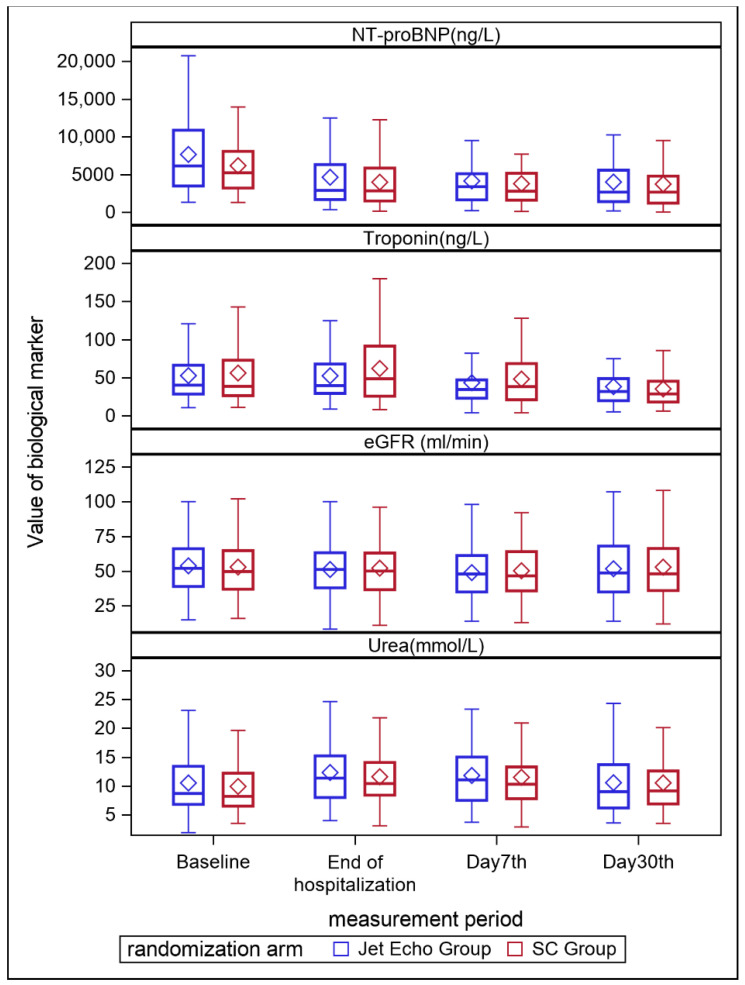
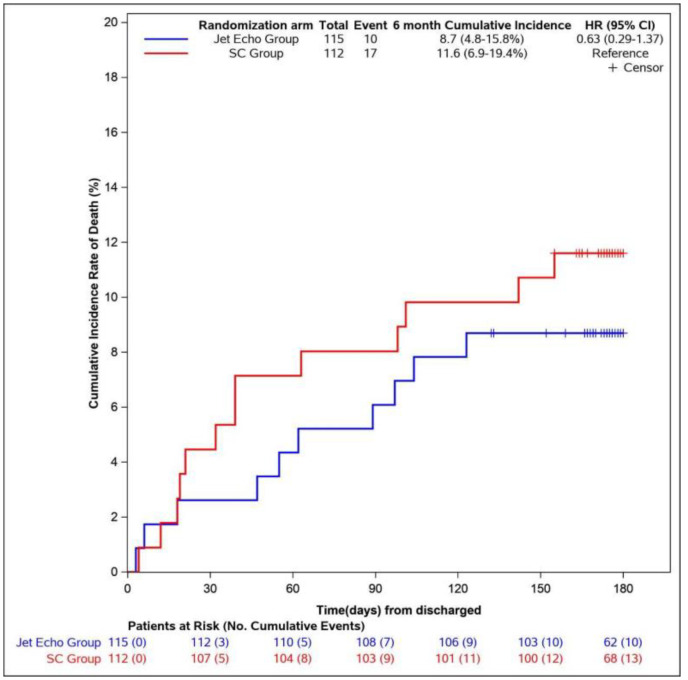
Acute heart failure (AHF) management is challenging, with high morbidity and readmission rates. There is little evidence of the benefit of HF monitoring during hospitalization. The aim of the study was to assess whether daily bedside echocardiographic monitoring (JetEcho) improved outcomes in AHF. In this prospective, open, two parallel-arm study (clinicaltrials.gov: NCT02892227), participants from two university hospitals were randomized to either standard of care (SC) or daily treatment adjustment including diuretics guided by JetEcho evaluating left ventricular filling pressure and volemia. The primary outcome was 30-day readmission rate. Key secondary outcomes were six-month cumulative incidence death, worsening HF during hospitalization and increasing of myocardial and renal biomarkers. From 250 included patients, 115 were finally analyzed in JetEcho group and 112 in SC group. Twenty-two (19%) patients were readmitted within 30 days in JetEcho group and 17 (15%) in SC group (relative risk [RR] 1.26; 95% confidence interval [CI], 0.70−2.24; p = 0.4). Worsening HF occurred in 17 (14%) patients in the JetEcho group and 24 (20%) in the SC group (RR 0.7; 95% [CI] 0.39 to 1.2; p = 0.2). No significant difference was found between the two groups concerning natriuretic peptides and renal function (p > 0.05 for all). The cumulative incidence rate of death from any cause at six months from discharge was 8.7% in the JetEcho group and 11.6% in the SC group (HR 0.63, 95% [CI] 0.3−1.4, p = 0.3). In AHF patients, a systematic daily bedside echocardiographic monitoring did not reduce 30-day readmission rate for HF and short-term clinical outcomes.
Keywords: acute heart failure; bedside echocardiography; cardiac filling pressure; congestion; readmissions.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Tuppin P., Cuerq A., de Peretti C., Fagot-Campagna A., Danchin N., Juillière Y., Alla F., Allemand H., Bauters C., Drici M.D., et al. Two-year outcome of patients after a first hospitalization for heart failure: A national observational study. Arch. Cardiovasc. Dis. 2014;107:158–168. doi: 10.1016/j.acvd.2014.01.012. - DOI - PubMed
-
- Conrad N., Judge A., Tran J., Mohseni H., Hedgecott D., Crespillo A.P., Allison M., Hemingway H., Cleland J.G., McMurray J.J., et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet Lond. Engl. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
