

A Shared Nephroprotective Mechanism for Renin-Angiotensin-System Inhibitors, Sodium-Glucose Co-Transporter 2 Inhibitors, and Vasopressin Receptor Antagonists: Immunology Meets Hemodynamics
- PMID: 35409276
- PMCID: PMC8999762
- DOI: 10.3390/ijms23073915
A Shared Nephroprotective Mechanism for Renin-Angiotensin-System Inhibitors, Sodium-Glucose Co-Transporter 2 Inhibitors, and Vasopressin Receptor Antagonists: Immunology Meets Hemodynamics
Abstract
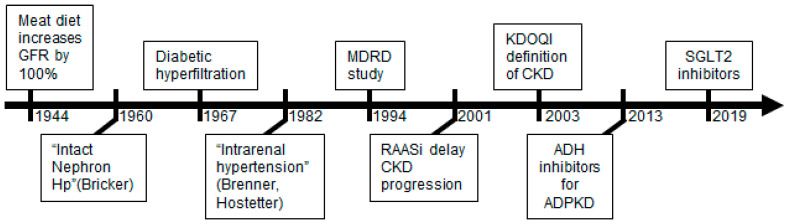
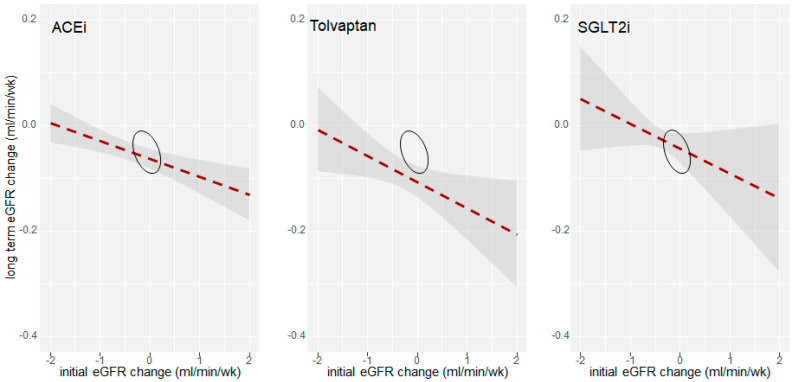
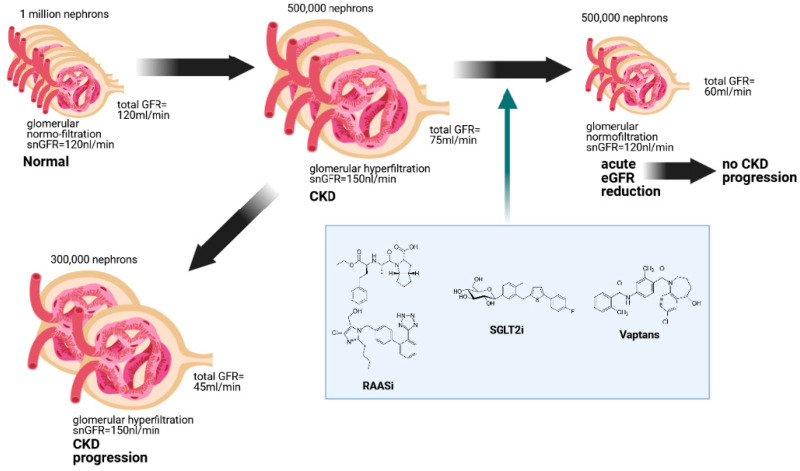
A major paradigm in nephrology states that the loss of filtration function over a long time is driven by a persistent hyperfiltration state of surviving nephrons. This hyperfiltration may derive from circulating immunological factors. However, some clue about the hemodynamic effects of these factors derives from the effects of so-called nephroprotective drugs. Thirty years after the introduction of Renin-Angiotensin-system inhibitors (RASi) into clinical practice, two new families of nephroprotective drugs have been identified: the sodium-glucose cotransporter 2 inhibitors (SGLT2i) and the vasopressin receptor antagonists (VRA). Even though the molecular targets of the three-drug classes are very different, they share the reduction in the glomerular filtration rate (GFR) at the beginning of the therapy, which is usually considered an adverse effect. Therefore, we hypothesize that acute GFR decline is a prerequisite to obtaining nephroprotection with all these drugs. In this study, we reanalyze evidence that RASi, SGLT2i, and VRA reduce the eGFR at the onset of therapy. Afterward, we evaluate whether the extent of eGFR reduction correlates with their long-term efficacy. The results suggest that the extent of initial eGFR decline predicts the nephroprotective efficacy in the long run. Therefore, we propose that RASi, SGLT2i, and VRA delay kidney disease progression by controlling maladaptive glomerular hyperfiltration resulting from circulating immunological factors. Further studies are needed to verify their combined effects.
Keywords: GFR; RASi; SGLT2i; chronic kidney disease; vaptans.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Nephroprotective effect of SGLT2 inhibitors in elderly patients with type 2 diabetes mellitus and hypertension: a real-world population-based cohort study.Postgrad Med. 2024 Nov;136(8):855-863. doi: 10.1080/00325481.2024.2426442. Epub 2024 Nov 13. Postgrad Med. 2024. PMID: 39513220
-
Use of renin angiotensin system inhibitors in patients with chronic kidney disease.Intern Med J. 2016 May;46(5):626-30. doi: 10.1111/imj.13060. Intern Med J. 2016. PMID: 27170242
-
Renoprotective effects of sodium glucose cotransporter 2 inhibitors in type 2 diabetes patients with decompensated heart failure.BMC Cardiovasc Disord. 2021 Jul 21;21(1):347. doi: 10.1186/s12872-021-02163-7. BMC Cardiovasc Disord. 2021. PMID: 34289813 Free PMC article.
-
Nephroprotection by SGLT2 Inhibition: Back to the Future?J Clin Med. 2020 Jul 15;9(7):2243. doi: 10.3390/jcm9072243. J Clin Med. 2020. PMID: 32679744 Free PMC article. Review.
-
Sodium-Glucose Cotransporter-2 Inhibition and the Glomerulus: A Review.Adv Ther. 2016 Sep;33(9):1502-18. doi: 10.1007/s12325-016-0379-5. Epub 2016 Jul 16. Adv Ther. 2016. PMID: 27423646 Free PMC article. Review.
Cited by
-
Renoprotective Effects of Tanshinone IIA: A Literature Review.Molecules. 2023 Feb 20;28(4):1990. doi: 10.3390/molecules28041990. Molecules. 2023. PMID: 36838978 Free PMC article. Review.
-
Cardiovascular-Kidney-Metabolic Effects: Steroidal and Nonsteroidal Mineralocorticoid Receptor Antagonists.Rev Cardiovasc Med. 2025 Jul 29;26(7):38690. doi: 10.31083/RCM38690. eCollection 2025 Jul. Rev Cardiovasc Med. 2025. PMID: 40776944 Free PMC article. Review.
-
SGLT2 Inhibition via Empagliflozin Improves Endothelial Function and Reduces Mitochondrial Oxidative Stress: Insights From Frail Hypertensive and Diabetic Patients.Hypertension. 2022 Aug;79(8):1633-1643. doi: 10.1161/HYPERTENSIONAHA.122.19586. Epub 2022 Jun 15. Hypertension. 2022. PMID: 35703100 Free PMC article.
-
Research Progress on the Positive and Negative Regulatory Effects of Rhein on the Kidney: A Review of Its Molecular Targets.Molecules. 2022 Oct 4;27(19):6572. doi: 10.3390/molecules27196572. Molecules. 2022. PMID: 36235108 Free PMC article. Review.
-
SGLT2 Inhibitors: The First Endothelial-Protector for Diabetic Nephropathy.J Clin Med. 2025 Feb 13;14(4):1241. doi: 10.3390/jcm14041241. J Clin Med. 2025. PMID: 40004772 Free PMC article. Review.
References
-
- Platt R. Sodium and potassium excretion in chronic renal failure. Clin. Sci. 1950;9:367–377. - PubMed
-
- Brenner B.M., Cooper M.E., de Zeeuw D., Keane W.F., Mitch W.E., Parving H.H., Remuzzi G., Snapinn S.M., Zhang Z., Shahinfar S., et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N. Engl. J. Med. 2001;345:861–869. doi: 10.1056/NEJMoa011161. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
