

A protocol for periprosthetic joint infections from the Northern Infection Network for Joint Arthroplasty (NINJA) in the Netherlands
- PMID: 35410299
- PMCID: PMC8996586
- DOI: 10.1186/s42836-022-00116-9
A protocol for periprosthetic joint infections from the Northern Infection Network for Joint Arthroplasty (NINJA) in the Netherlands
Abstract
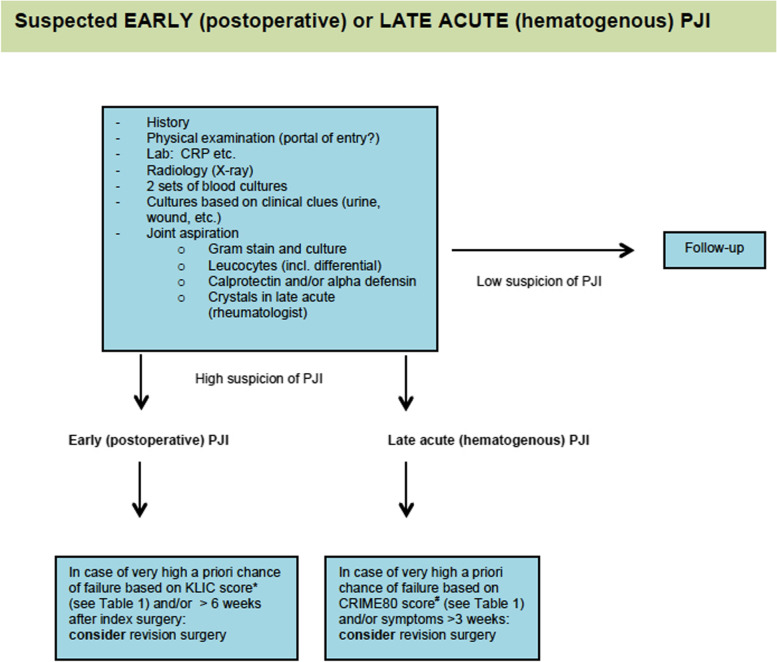
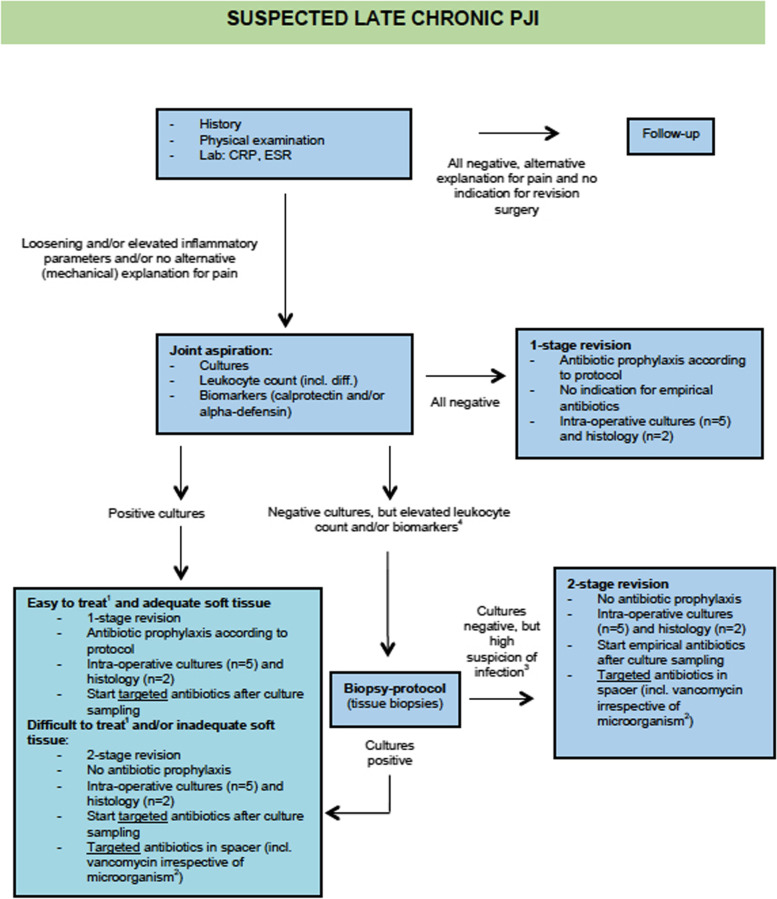
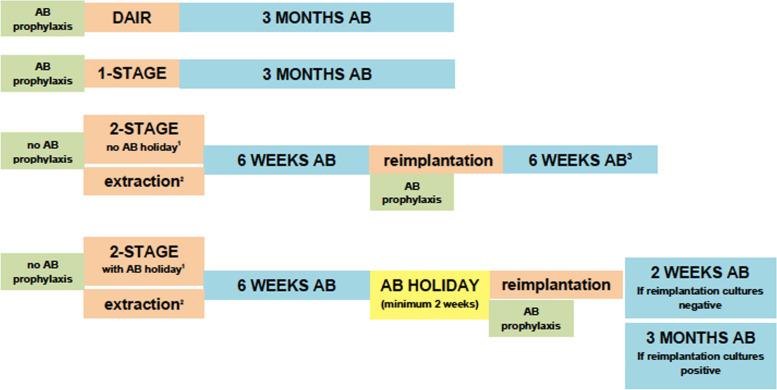
Periprosthetic joint infection (PJI) is a devastating complication of joint arthroplasty surgery. Treatment success depends on accurate diagnostics, adequate surgical experience and interdisciplinary consultation between orthopedic surgeons, plastic surgeons, infectious disease specialists and medical microbiologists. For this purpose, we initiated the Northern Infection Network for Joint Arthroplasty (NINJA) in the Netherlands in 2014. The establishment of a mutual diagnostic and treatment protocol for PJI in our region has enabled mutual understanding, has supported agreement on how to treat specific patients, and has led to clarity for smaller hospitals in our region for when to refer patients without jeopardizing important initial treatment locally. Furthermore, a mutual PJI patient database has enabled the improvement of our protocol, based on medicine-based evidence from our scientific data. In this paper we describe our NINJA protocol.Level of evidence: III.
Keywords: Arthroplasty Surgery; Debridement Antibiotics and Implant Retention (DAIR); Periprosthetic joint infection (PJI); Protocol; Treatment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests and they were not involved in the journal’s review of or decisions related to, this manuscript.
Figures
References
-
- Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, Garvin KL, Mont MA, Wongworawat MD, Zalavras CG. New definition for periprosthetic joint infection: from the Workgroup of the Musculoskeletal Infection Society. Clin Orthop Relat Res. 2011;469:2992–2994. doi: 10.1007/s11999-011-2102-9. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources