

Effects of experimentally induced cervical spine mobility alteration on the postural organisation of gait initiation
- PMID: 35410364
- PMCID: PMC9001680
- DOI: 10.1038/s41598-022-10101-6
Effects of experimentally induced cervical spine mobility alteration on the postural organisation of gait initiation
Abstract
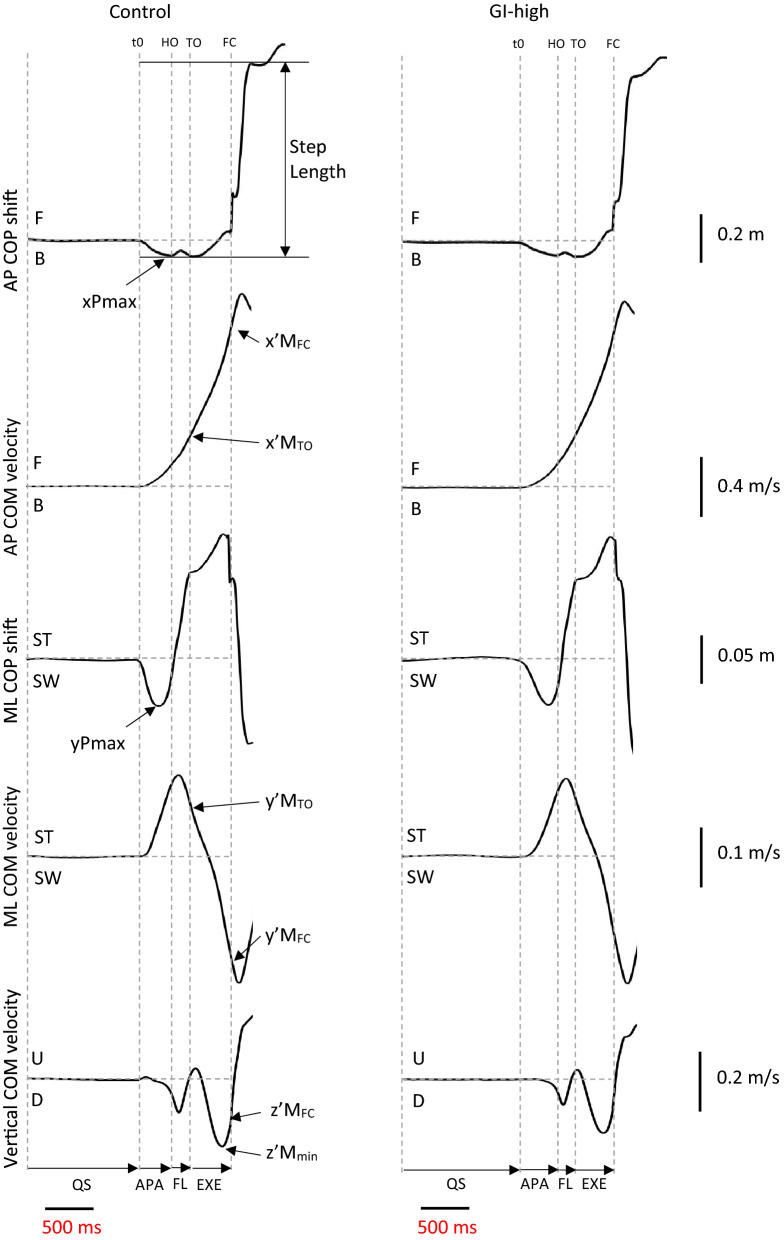
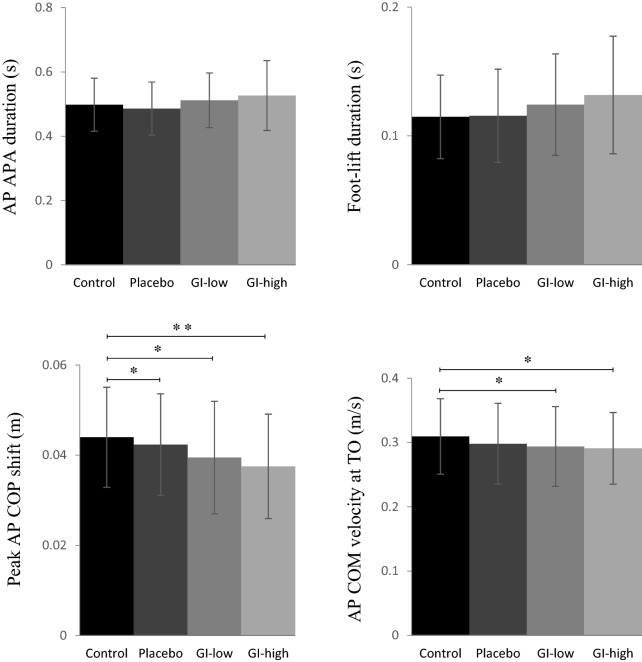
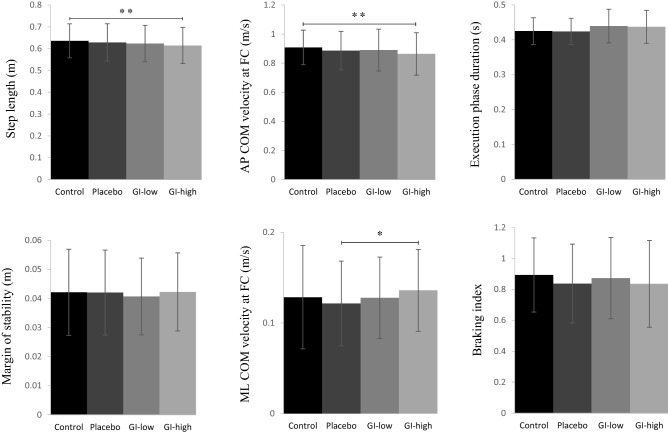
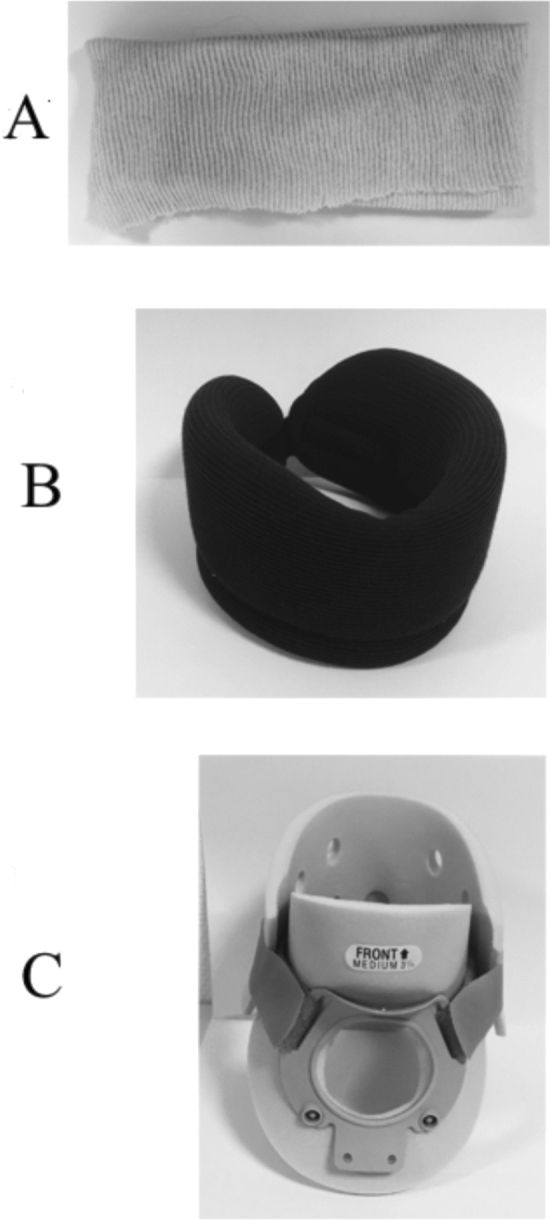
Gait initiation (GI), the transient period between quiet standing and locomotion, is a functional task classically used in the literature to investigate postural control. This study aimed to investigate the influence of an experimentally-induced alteration of cervical spine mobility (CSM) on GI postural organisation. Fifteen healthy young adults initiated gait on a force-plate in (1) two test conditions, where participants wore a neck orthosis that passively simulated low and high levels of CSM alteration; (2) one control condition, where participants wore no orthosis; and (3) one placebo condition, where participants wore a cervical bandage that did not limit CSM. Centre-of-pressure and centre-of-mass kinematics were computed based on force-plate recordings according to Newton's second law. Main results showed that anticipatory postural adjustments amplitude (peak backward centre-of-pressure shift and forward centre-of-mass velocity at toe-off) and motor performance (step length and forward centre-of-mass velocity at foot-contact) were altered under the condition of high CSM restriction. These effects of CSM restriction may reflect the implementation of a more cautious strategy directed to attenuate head-in-space destabilisation and ease postural control. It follows that clinicians should be aware that the prescription of a rigid neck orthosis to posturo-deficient patients could exacerbate pre-existing GI deficits.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Le Bozec, S. & Bouisset, S. Posturo-kinetic capacity and postural function in voluntary movements. Progress in Motor Control, Volume Two: Structure-Function Relations in Voluntary Movements 25–52 (Human Kinetics, 2002).
-
- Belen’kiĭ VE, Gurfinkel’ VS, Paltsev EI. Control elements of voluntary movements. Biofizika. 1967;12:135–141. - PubMed
-
- Bouisset S, Zattara M. A sequence of postural movements precedes voluntary movement. Neurosci. Lett. 1981;22:263–270. doi: 10.1016/0304-3940(81)90117-8. - DOI
-
- Massion J. Postural changes accompanying voluntary movements. Normal and pathological aspects. Hum Neurobiol. 1984;2:261–267. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
