

Detection of astrocytic tau pathology facilitates recognition of chronic traumatic encephalopathy neuropathologic change
- PMID: 35410438
- PMCID: PMC8996534
- DOI: 10.1186/s40478-022-01353-4
Detection of astrocytic tau pathology facilitates recognition of chronic traumatic encephalopathy neuropathologic change
Abstract
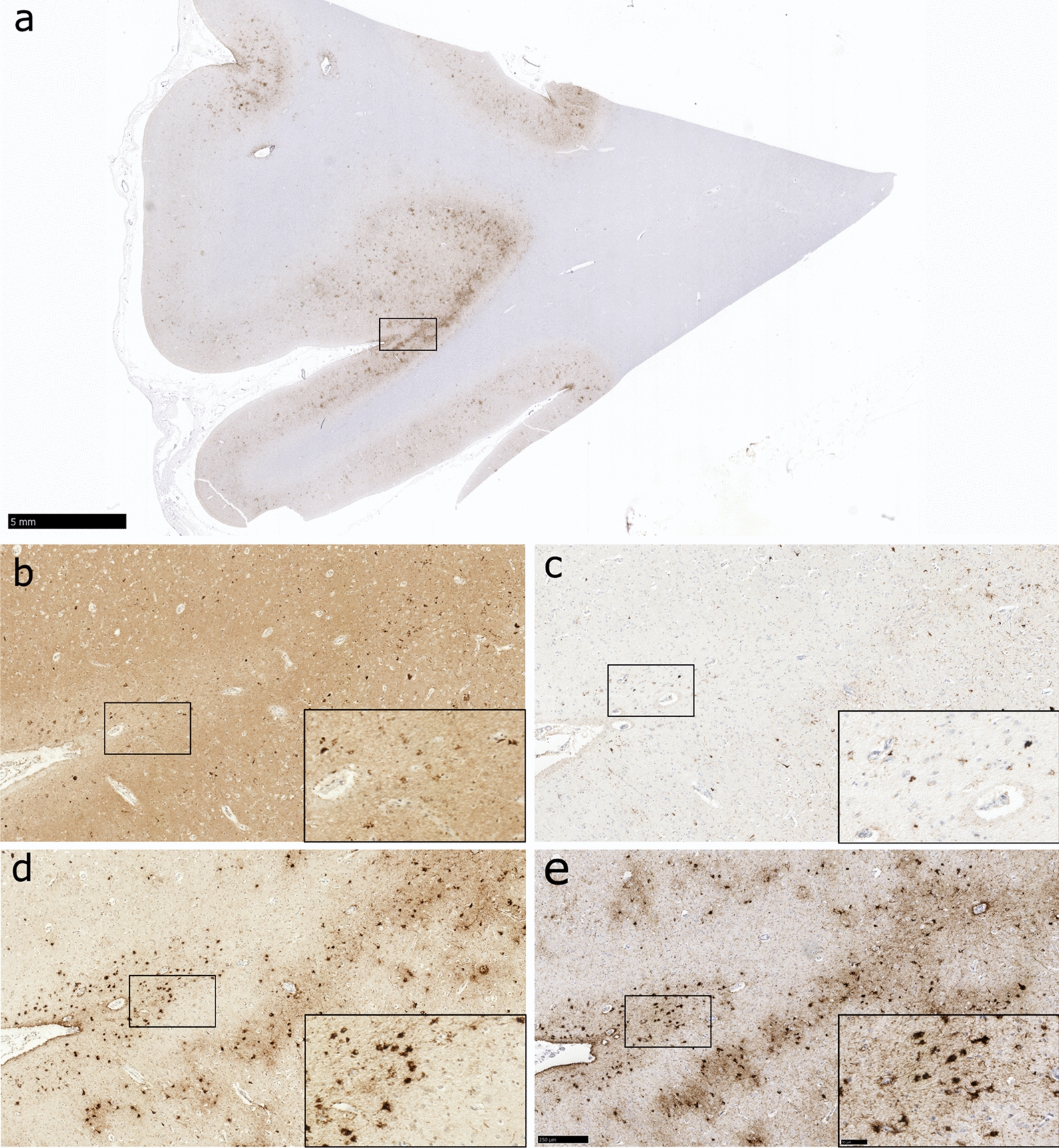
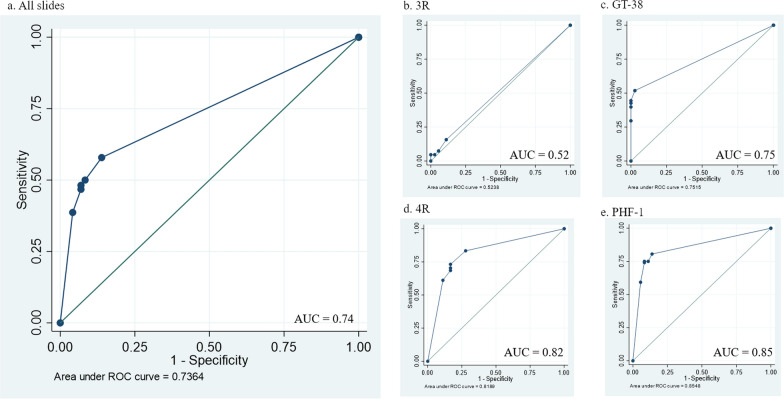
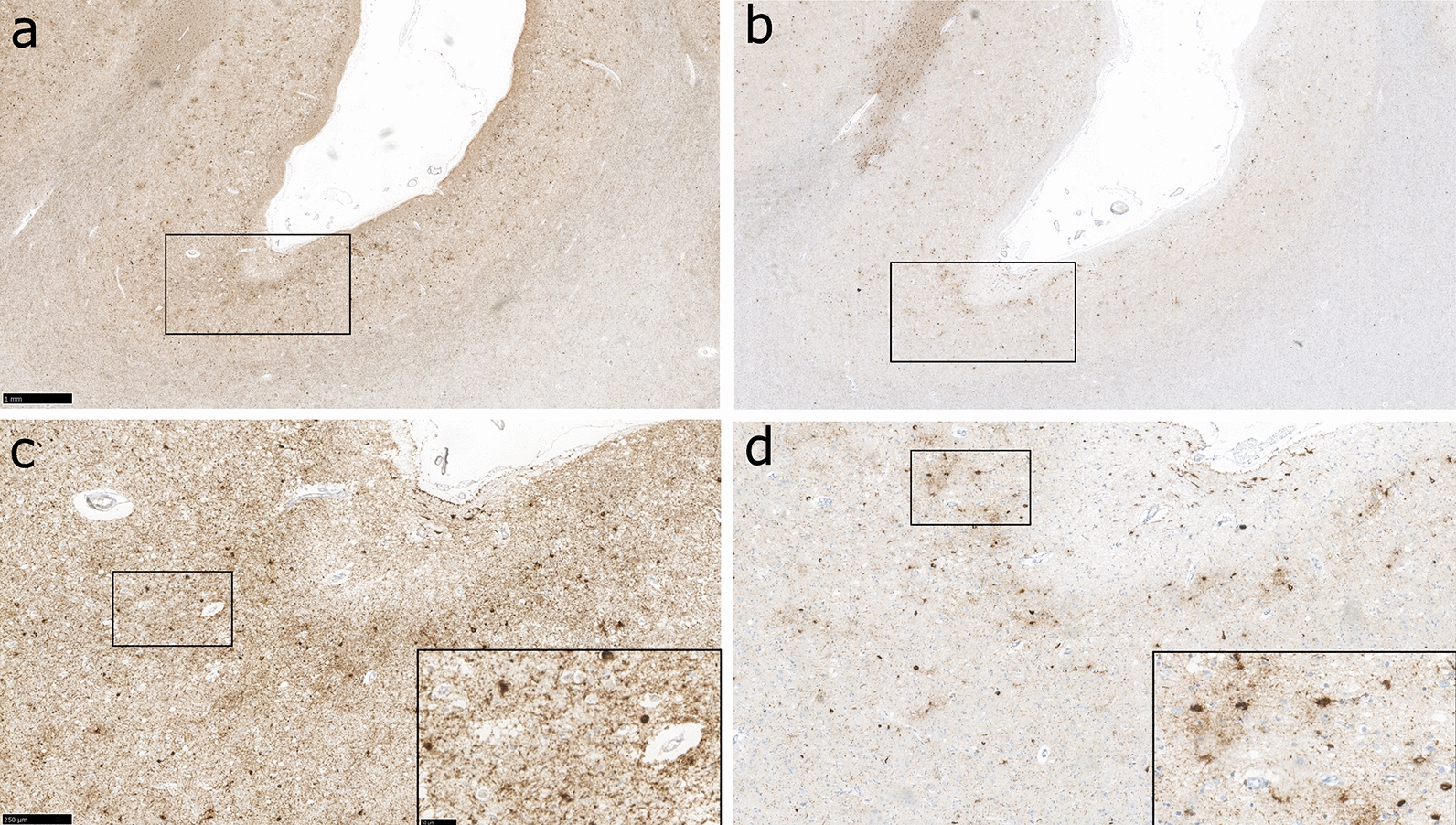
Traumatic brain injury (TBI) is associated with the development of a range of neurodegenerative pathologies, including chronic traumatic encephalopathy (CTE). Current consensus diagnostic criteria define the pathognomonic cortical lesion of CTE neuropathologic change (CTE-NC) as a patchy deposition of hyperphosphorylated tau in neurons, with or without glial tau in thorn-shaped astrocytes, typically towards the depths of sulci and clustered around small blood vessels. Nevertheless, although incorporated into consensus diagnostic criteria, the contribution of the individual cellular components to identification of CTE-NC has not been formally evaluated. To address this, from the Glasgow TBI Archive, cortical tissue blocks were selected from consecutive brain donations from contact sports athletes in which there was known to be either CTE-NC (n = 12) or Alzheimer's disease neuropathologic change (n = 4). From these tissue blocks, adjacent tissue sections were stained for tau antibodies selected to reveal either solely neuronal pathology (3R tau; GT-38) or mixed neuronal and astroglial pathologies (4R tau; PHF-1). These stained sections were then randomised and independently assessed by a panel of expert neuropathologists, blind to patient clinical history and primary antibody applied to each section, who were asked to record whether CTE-NC was present. Results demonstrate that, in sections stained for either 4R tau or PHF-1, consensus recognition of CTE-NC was high. In contrast, recognition of CTE-NC in sections stained for 3R tau or GT-38 was poor; in the former no better than chance. Our observations demonstrate that the presence of both neuronal and astroglial tau pathologies facilitates detection of CTE-NC, with its detection less consistent when neuronal tau pathology alone is visible. The combination of both glial and neuronal pathologies, therefore, may be required for detection of CTE-NC.
Keywords: Aging-related tau astrogliopathy; Chronic traumatic encephalopathy; Neurodegeneration; Tau; Traumatic brain injury.
© 2022. The Author(s).
Conflict of interest statement
The authors report no competing interests.
Figures
References
-
- Brandenburg W, Hallervorden J. Dementia pugilistica with anatomical findings [German]. Virchows Arch. Pathol Anat Physiol Klin Med. 1954;325:680–709. - PubMed
-
- Bieniek KF, Cairns NJ, Crary JF, Dickson DW, Folkerth RD, Keene CD, Litvan I, Perl DP, Stein TD, Vonsattel J-P, Stewart W, Dams-O’Connor K, Gordon WA, Tripodis Y, Alvarez VE, Mez J, Alosco ML, McKee AC, TBI/CTE Research Group The second NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. J Neuropathol Exp Neurol. 2021;80(3):210–219. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
