

Predictors of severe illness in children with multisystem inflammatory syndrome after SARS-CoV-2 infection: a multicentre cohort study
- PMID: 35410860
- PMCID: PMC9001008
- DOI: 10.1503/cmaj.210873
Predictors of severe illness in children with multisystem inflammatory syndrome after SARS-CoV-2 infection: a multicentre cohort study
Abstract
Background: SARS-CoV-2 infection can lead to multisystem inflammatory syndrome in children (MIS-C). We sought to investigate risk factors for admission to the intensive care unit (ICU) and explored changes in disease severity over time.
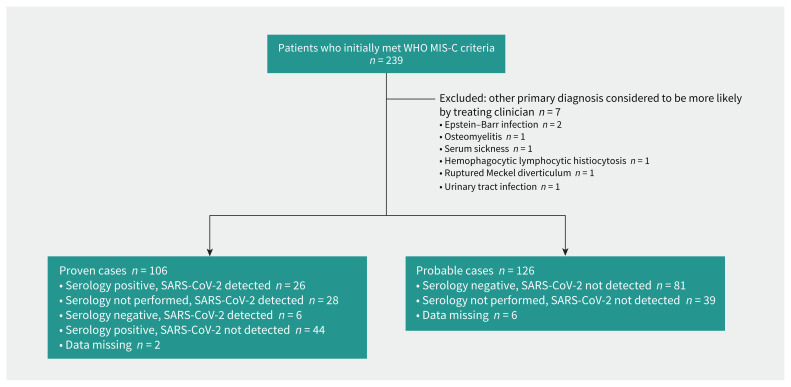
Methods: We obtained data from chart reviews of children younger than 18 years with confirmed or probable MIS-C who were admitted to 15 hospitals in Canada, Iran and Costa Rica between Mar. 1, 2020, and Mar. 7, 2021. Using multivariable analyses, we evaluated whether admission date and other characteristics were associated with ICU admission or cardiac involvement.
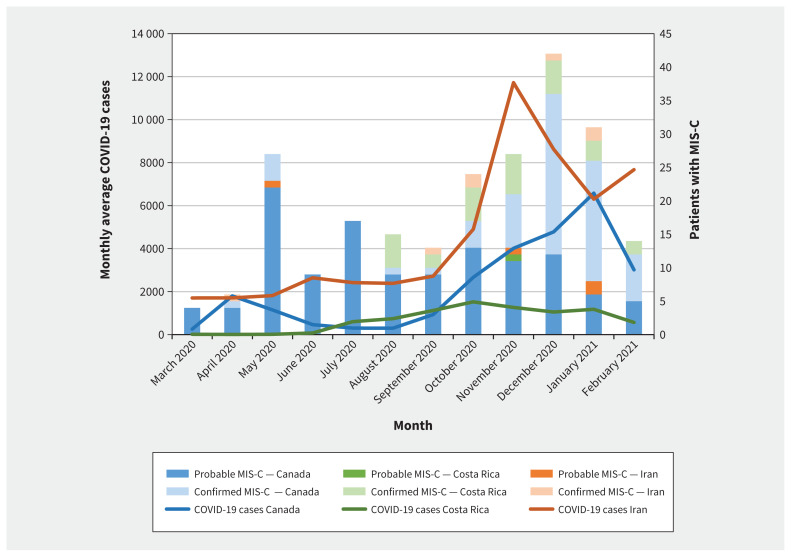
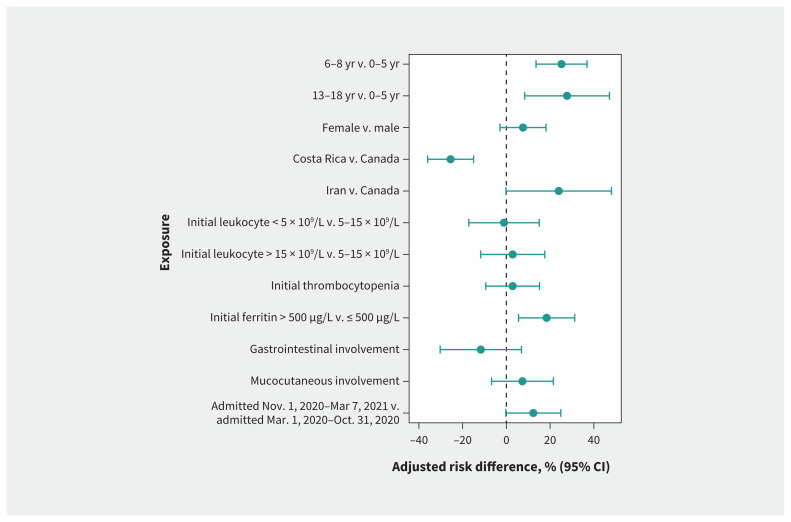
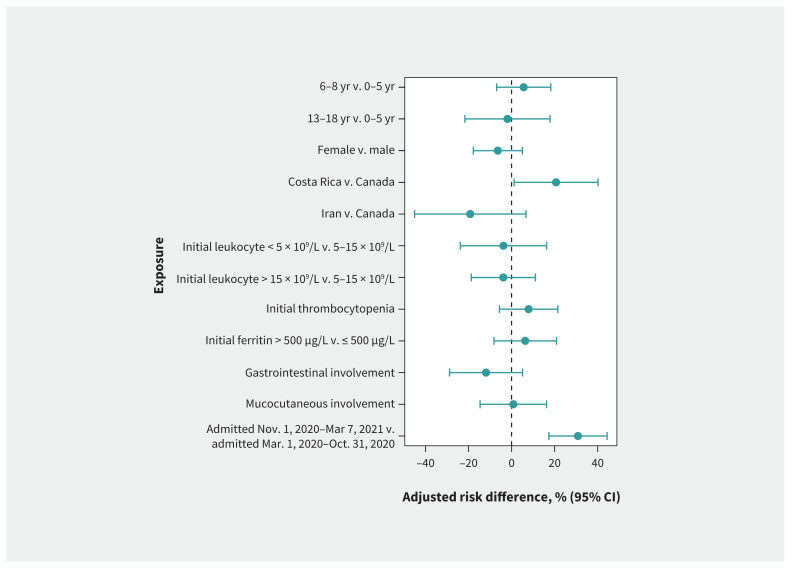
Results: Of 232 children with MIS-C (median age 5.8 yr), 130 (56.0%) were male and 50 (21.6%) had comorbidities. Seventy-three (31.5%) patients were admitted to the ICU but none died. We observed an increased risk of ICU admission among children aged 13-17 years (adjusted risk difference 27.7%, 95% confidence interval [CI] 8.3% to 47.2%), those aged 6-12 years (adjusted risk difference 25.2%, 95% CI 13.6% to 36.9%) or those with initial ferritin levels greater than 500 μg/L (adjusted risk difference 18.4%, 95% CI 5.6% to 31.3%). Children admitted to hospital after Oct. 31, 2020, had numerically higher rates of ICU admission (adjusted risk difference 12.3%, 95% CI -0.3% to 25.0%) and significantly higher rates of cardiac involvement (adjusted risk difference 30.9%, 95% CI 17.3% to 44.4%). At Canadian sites, the risk of ICU admission was significantly higher for children admitted to hospital between December 2020 and March 2021 than those admitted between March and May 2020 (adjusted risk difference 25.3%, 95% CI 6.5% to 44.0%).
Interpretation: We observed that age and higher ferritin levels were associated with more severe MIS-C. We observed greater severity of MIS-C later in the study period. Whether emerging SARS-CoV-2 variants pose different risks of severe MIS-C needs to be determined.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Joanna Merckx reports a role as medical director of bioMerieux Canada and as a volunteer member of the Belgian Pediatric Task Force for COVID-19 during the conduct of the study. She is also an independent researcher, with a contract with Public Health Belgium, Sciensano for a study on the seroprevalence of SARS-CoV-2 in schools. E. Ann Yeh reports grants from Biogen, Roche, Horizon Therapeutics and Alexion; honoraria from Prime and Novartis; and participation on advisory boards with Roche and Horizon Therapeutics. She is also involved with the editorial board or is an editor with Multiple Sclerosis and Related Disorders, Multiple Sclerosis Journal, PLOS ONE and Neurology. Jesse Papenburg reports grants from AbbVie, Sanofi Pasteur, Merck and MedImmune; consulting fees from Merck; and honoraria from AbbVie, AstraZeneca and Seegene. He is a member of the National Advisory Committee on Immunization. Marie-Astrid Lefebvre reports an honorarium from Takeda Canada. Tammie Dewan reports grants from the Sick Kids Hospital Foundation, the Canadian Institutes for Health Research (CIHR) and the Department of Pediatrics at the University of Calgary. She is a past president of the Complex Care Section of the Canadian Pediatric Society. Jared Bullard reports grants from CIHR, the Manitoba Medical Service Foundation and Research Manitoba, as well as participation on provincial and hospital leadership committees. He is also secretary of the Association of Medical Microbiology and Infectious Diseases. Manish Sadarangani reports grants from GlaxoSmithKline, Merck, Moderna, Pfizer, Sanofi Pasteur, Seqirus, Symvivo and VBI Vaccines, as well as participating on 2 data safety monitoring boards for COVID-19 vaccine trials. Rupeena Purewal reports honoraria and consulting fees from Verity Pharmaceuticals. Kirk Leifso reports a grant from the Hospital for Sick Children. Cheryl Foo reports an unpaid position with IMPACT. No other competing interests were declared.
Figures
References
-
- Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19 [scientific brief]. Geneva: World Health Organization; 2020. Available: https://www.who.int/news-room/commentaries/detail/multisystem-inflammato... (accessed 2021 May 10).
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous