

Prediction of Naming Outcome With fMRI Language Lateralization in Left Temporal Epilepsy Surgery
- PMID: 35410903
- PMCID: PMC9202528
- DOI: 10.1212/WNL.0000000000200552
Prediction of Naming Outcome With fMRI Language Lateralization in Left Temporal Epilepsy Surgery
Abstract
Background and objectives: Naming decline after left temporal lobe epilepsy (TLE) surgery is common and difficult to predict. Preoperative language fMRI may predict naming decline, but this application is still lacking evidence. We performed a large multicenter cohort study of the effectiveness of fMRI in predicting naming deficits after left TLE surgery.
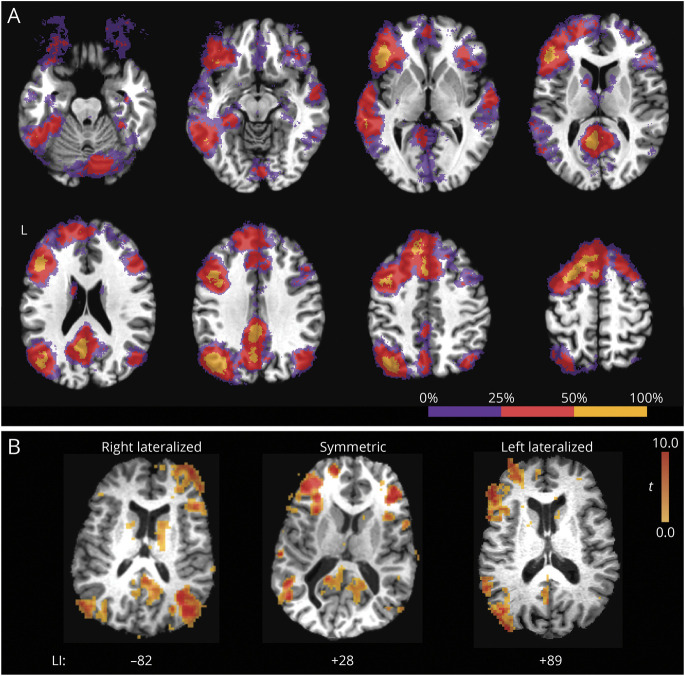
Methods: At 10 US epilepsy centers, 81 patients with left TLE were prospectively recruited and given the Boston Naming Test (BNT) before and ≈7 months after anterior temporal lobectomy. An fMRI language laterality index (LI) was measured with an auditory semantic decision-tone decision task contrast. Correlations and a multiple regression model were built with a priori chosen predictors.
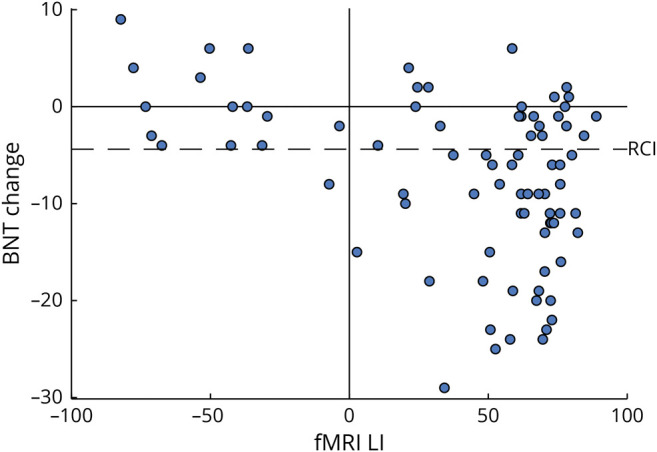
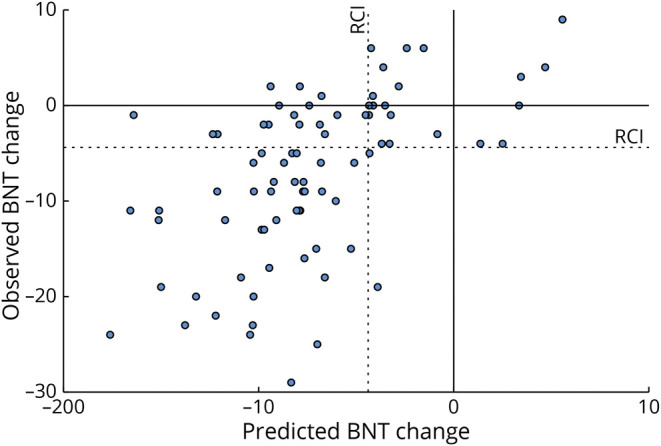
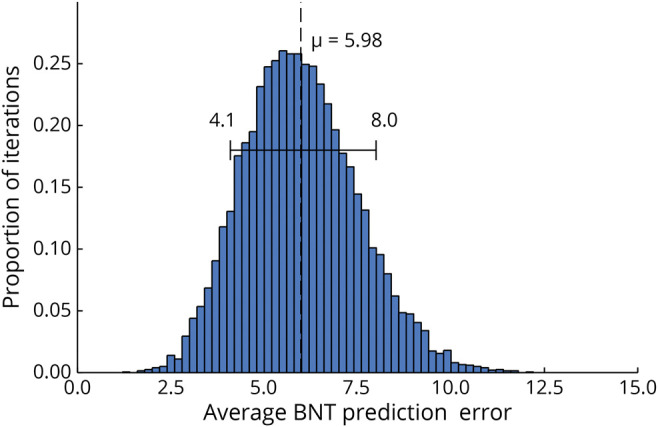
Results: Naming decline occurred in 56% of patients and correlated with fMRI LI (r = -0.41, p < 0.001), age at epilepsy onset (r = -0.30, p = 0.006), age at surgery (r = -0.23, p = 0.039), and years of education (r = 0.24, p = 0.032). Preoperative BNT score and duration of epilepsy were not correlated with naming decline. The regression model explained 31% of the variance, with fMRI contributing 14%, with a 96% sensitivity and 44% specificity for predicting meaningful naming decline. Cross-validation resulted in an average prediction error of 6 points.
Discussion: An fMRI-based regression model predicted naming outcome after left TLE surgery in a large, prospective multicenter sample, with fMRI as the strongest predictor. These results provide evidence supporting the use of preoperative language fMRI to predict language outcome in patients undergoing left TLE surgery.
Classification of evidence: This study provides Class I evidence that fMRI language lateralization can help in predicting naming decline after left TLE surgery.
© 2022 American Academy of Neurology.
Figures
Comment in
-
fMRI Has Added Value in Predicting Naming After Epilepsy Surgery.Neurology. 2022 Jun 7;98(23):959-960. doi: 10.1212/WNL.0000000000200328. Epub 2022 Apr 11. Neurology. 2022. PMID: 35410901 No abstract available.
-
fMRI to Predict Naming Decline: Can We Improve the Grade From a C to an A?Epilepsy Curr. 2022 Sep 22;22(6):345-347. doi: 10.1177/15357597221126277. eCollection 2022 Nov-Dec. Epilepsy Curr. 2022. PMID: 36426181 Free PMC article. No abstract available.
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001;345(5):311-318. - PubMed
-
- Téllez-Zenteno JF, Dhar R, Wiebe S. Long-term seizure outcomes following epilepsy surgery: a systematic review and meta-analysis. Brain. 2005;128:1188-1198. - PubMed
-
- Sherman EM, Wiebe S, Fay-McClymont TB, et al. . Neuropsychological outcomes after epilepsy surgery: systematic review and pooled estimates. Epilepsia. 2011;52(5):857-869. - PubMed
-
- Perrine K, Hermann BP, Meador KJ, et al. . The relationship of neuropsychological functioning to quality of life in epilepsy. Arch Neurol. 1995;52(10):997-1003. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials