

Prevalence and Patient Outcomes of Adult Primary Hypercholesterolemia and Dyslipidemia in the UK: Longitudinal Retrospective Study Using a Primary Care Dataset from 2009 to 2019
- PMID: 35411162
- PMCID: PMC8994561
- DOI: 10.2147/CEOR.S347085
Prevalence and Patient Outcomes of Adult Primary Hypercholesterolemia and Dyslipidemia in the UK: Longitudinal Retrospective Study Using a Primary Care Dataset from 2009 to 2019
Abstract
Background: Guidelines for the management of dyslipidemias recommend intensive low-density lipoprotein (LDL-C) control through lifestyle advice and lipid-lowering drugs to reduce the risk of cardiovascular disease (CVD).
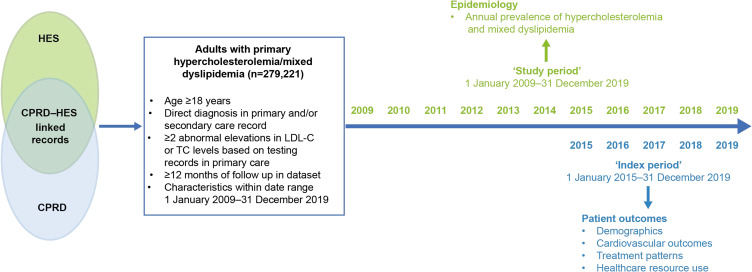
Objective: This retrospective study aimed to characterize the adult primary care population with primary hypercholesterolemia (PH)/mixed dyslipidemia (MD).
Methods: Data on adults with PH/MD between 1 January 2009 and 31 December 2019 in the UK were extracted from linked primary Clinical Practice Research Datalink (CPRD) and secondary care (Hospital Episode Statistics) datasets and analyzed.
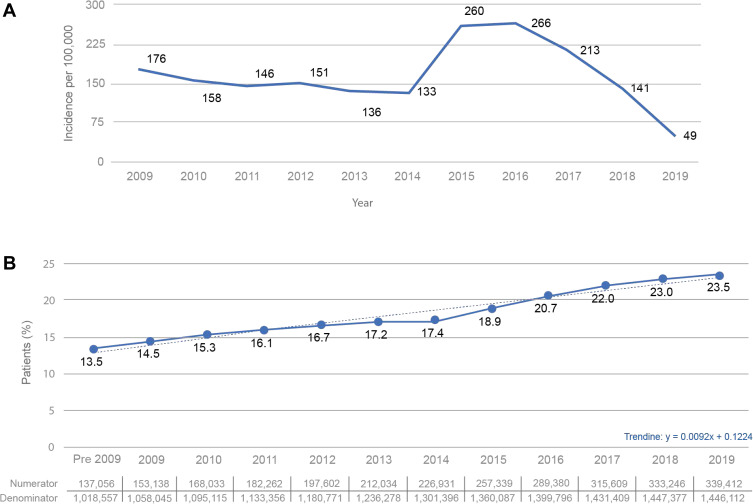
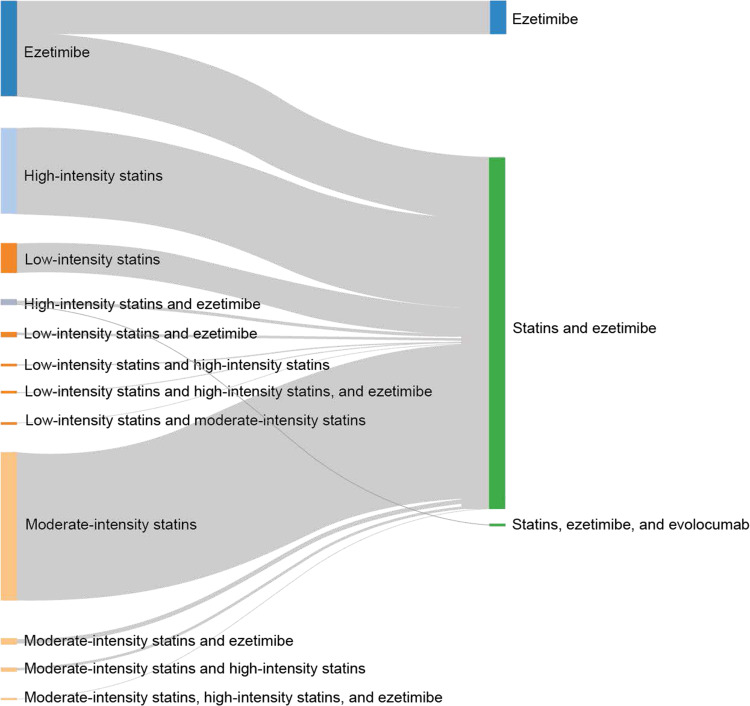
Results: A total of 279,221 patients met the inclusion criteria. Mean follow-up was 8.6 years. Crude prevalence of PH/MD increased from 13.5% in 2009 to 23.5% by 2019. The incidence decreased from 176 to 49 per 100,000 population. Mean age of the cohort was 58 years, baseline LDL-C was 4.32 mmol/L, 19.6% had atherosclerotic CVD, 30.1% diabetes, and 8.5% heterozygous familial hypercholesterolemia. Estimated LDL-C reductions of 40% and 50% were achieved in 2.6% and 2.3% of patients, respectively. Most received moderate-intensity statins as monotherapy (62.4%); high-intensity statins were used less frequently (24.3% as initial treatment). Less than 10% of patients received ezetimibe plus statins of different intensities.
Conclusion: The prevalence of dyslipidemia doubled between 2009 and 2019, likely due to more systematic identification of PH/MD. A large proportion of patients with PH/MD are of high and very high CV risk, remain suboptimally treated in terms of lipid lowering, and may experience CV events with associated non-negligible clinical and economic sequelae. Despite intensive LDL-C-lowering recommendations, these do not translate in clinical practice to the wider population.
Keywords: NICE guidelines; atherosclerosis; cardiovascular disease; lipid management.
© 2022 Bilitou et al.
Conflict of interest statement
Dr Aikaterini Bilitou and Dr Inaam Haq are employees of Daiichi Sankyo Europe GmbH. Kyle Dunton is an employee of Daiichi Sankyo UK. At the time of the study and manuscript preparation, John Were, Archie Farrer, Dr Simon Wan Yau Ming, and Dr Adrian Rabe were employees of Health iQ Ltd. Dr Adrian Rabe was also an honorary research fellow at Imperial College London. The authors report no other conflicts of interest in this work.
Figures
References
-
- British Heart Foundation. UK factsheet; 2021. Available from: www.bhf.org.uk/what-we-do/our-research/heart-statistics. Accessed May 3, 2021.
-
- European Heart Network. European Cardiovascular Disease Statistics: 2017 Edition. Brussels, Belgium: European Heart Network; 2017.
-
- Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
