

PIK-75 overcomes venetoclax resistance via blocking PI3K-AKT signaling and MCL-1 expression in mantle cell lymphoma
- PMID: 35411248
- PMCID: PMC8984906
PIK-75 overcomes venetoclax resistance via blocking PI3K-AKT signaling and MCL-1 expression in mantle cell lymphoma
Abstract
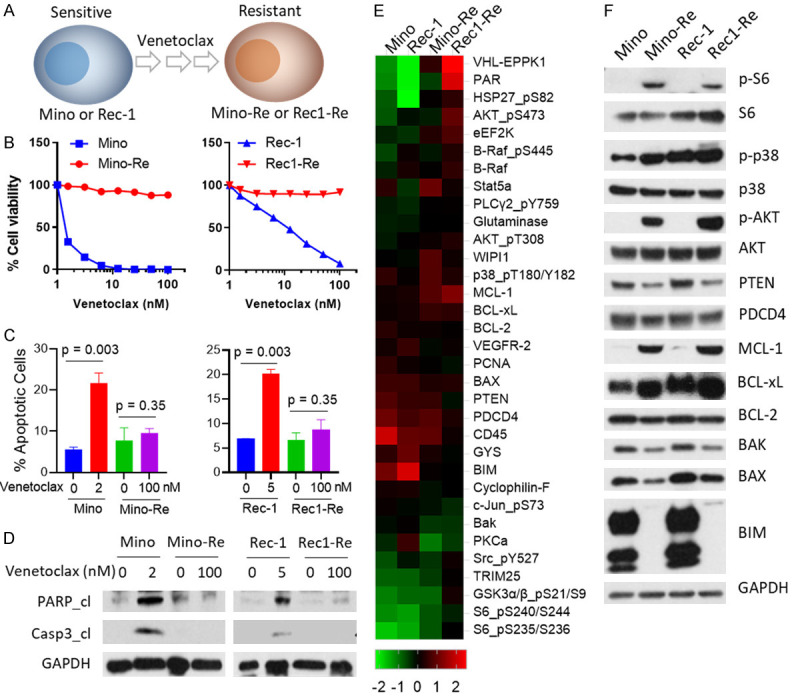
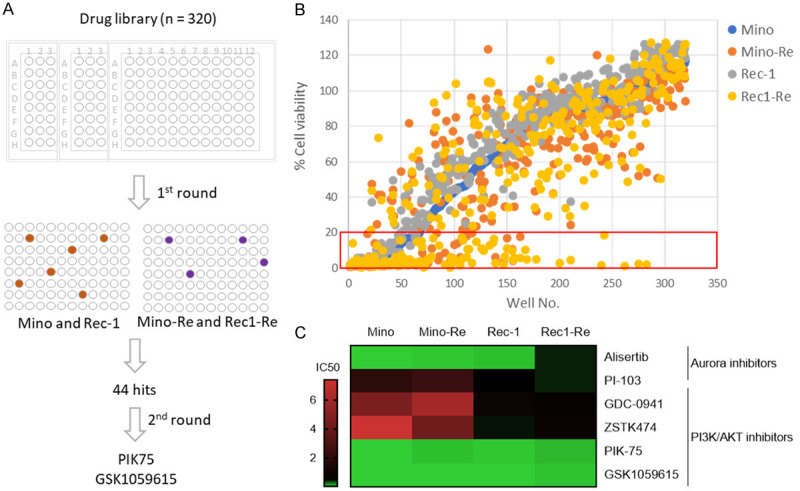
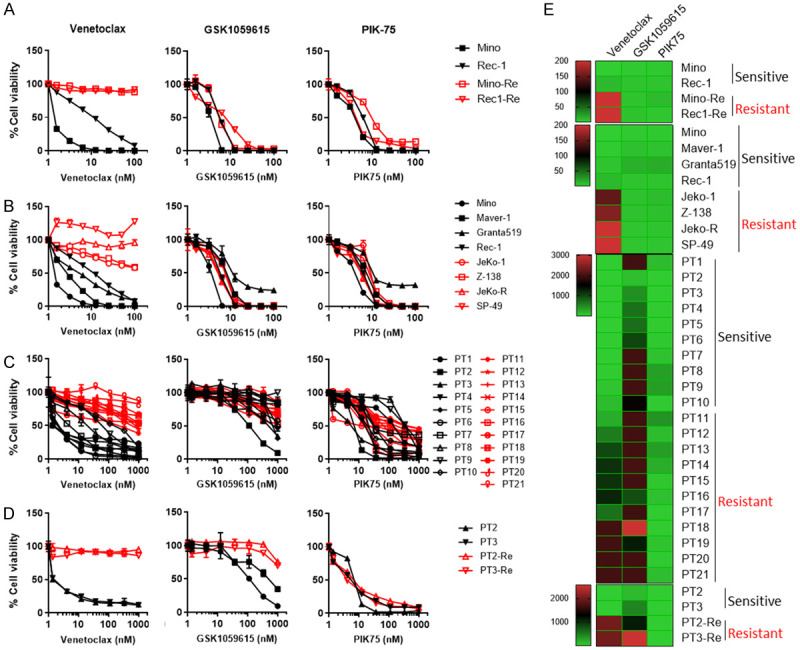
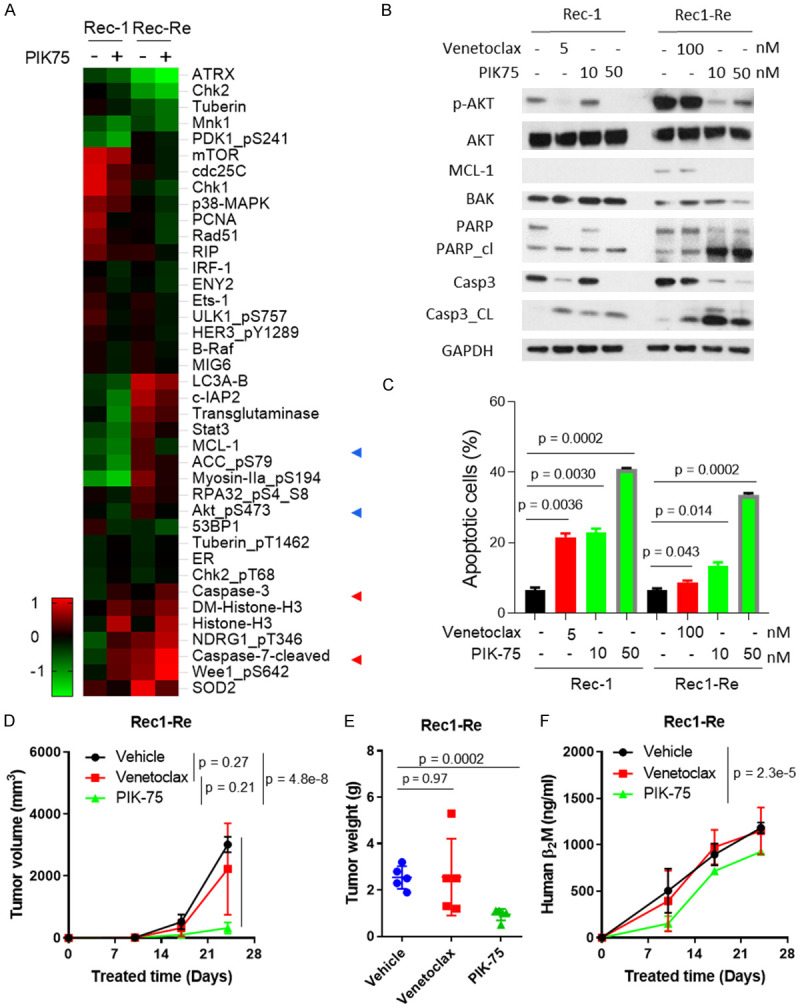
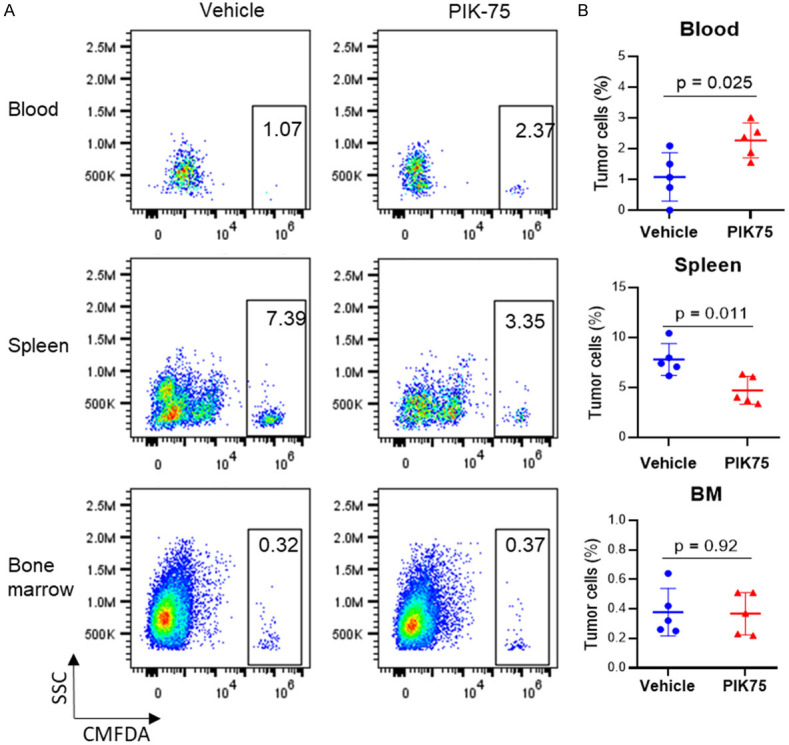
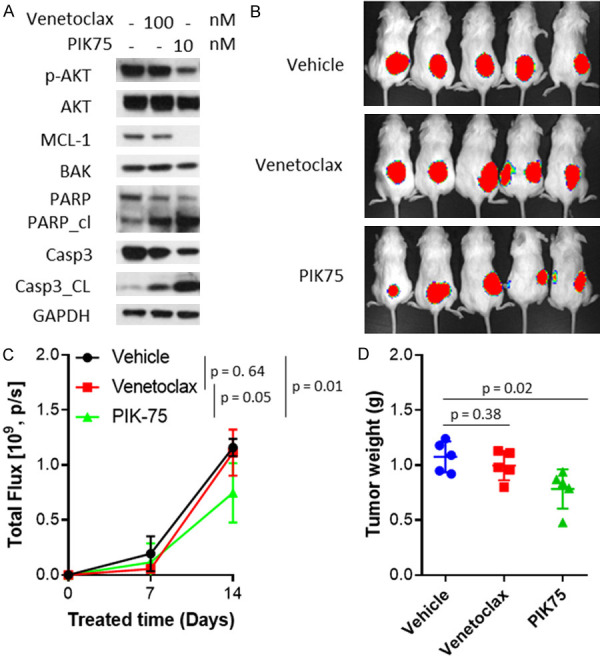
Therapeutic resistance is the major challenge in clinic for patients with mantle cell lymphoma (MCL), an aggressive subtype of B-cell lymphoma. In addition to the FDA-approved Bruton's tyrosine kinase (BTK) inhibitors, multiple clinical trials have demonstrated clinical benefits in targeting BCL-2 by venetoclax and reported to greatly improve clinical outcome for refractory/relapsed patients with MCL alone or in combination with BTK inhibitors. However, resistance to venetoclax is no exception and marks as a new clinic challenge. To decode the underlying mechanisms driving venetoclax resistance, we established two MCL cell lines, Mino-Re and Rec1-Re, with acquired resistance to venetoclax from sensitive Mino and Rec-1. Using reverse phase protein assay (RPPA), an agnostic proteomic approach, we identified targetable signaling pathways that are associated with acquired venetoclax resistance in Mino-Re and Rec1-Re cells. A panel of pro-survival signals was identified to correlate well with venetoclax-resistance, including increased expression of MCL-1, BCL-xL and AKT phosphorylation, and decreased expression of BIM, BAX and PTEN. Based on a high throughput drug screening of over 320 FDA-approved/investigational drugs in the paired venetoclax-sensitive and -resistant cell lines Mino-Re and Rec1-Re, we identified the top candidates that are capable to overcome acquired venetoclax resistance in these cells. The best candidate is PIK-75, a dual inhibitor targeting both PI3K and CDK9. Its action to overcome venetoclax resistance was further confirmed in additional cell lines with primary venetoclax resistance (n=4) and primary patient samples (n=21). Mechanistically, PIK75 treatment potently diminished the elevated MCL-1 expression and AKT activation in cells with acquired or primary venetoclax resistance and resulted in potent anti-MCL activity to overcome these resistances. In addition, PIK75 is also potent in overcoming tumor microenvironment (TME)-associated venetoclax resistance. Furthermore, PIK-75 treatment is efficacious in overcoming primary and acquired venetoclax resistance in xenograft models and inhibited tumor cell dissemination to spleen in mice. Altogether, our data demonstrated that PIK-75 is highly potent in overcoming primary, acquired, or stromal cells-induced venetoclax resistances in MCL cells and revealed a new tumor vulnerability that can be exploited clinically in difficult to treat MCL cases, especially those with venetoclax resistance.
Keywords: AKT; MCL-1; PI3K; PIK75; mantle cell lymphoma; venetoclax resistance.
AJCR Copyright © 2022.
Conflict of interest statement
M.W. is a consultant for: InnoCare, Loxo Oncology, Juno, Oncternal, CStone, AstraZeneca, Janssen, VelosBio, Pharmacyclics, Genentech, Bayer Healthcare. His research is funded by: Pharmacyclics, Janssen, AstraZeneca, Celgene, Loxo Oncology, Kite Pharma, Juno, BioInvent, VelosBio, Acerta Pharma, Oncternal, Verastem, Molecular Templates, Lilly, Innocare. All other authors declare no competing financial interests.
Figures
References
-
- Roberts AW, Davids MS, Pagel JM, Kahl BS, Puvvada SD, Gerecitano JF, Kipps TJ, Anderson MA, Brown JR, Gressick L, Wong S, Dunbar M, Zhu M, Desai MB, Cerri E, Heitner Enschede S, Humerickhouse RA, Wierda WG, Seymour JF. Targeting BCL2 with venetoclax in relapsed chronic lymphocytic leukemia. N Engl J Med. 2016;374:311–322. - PMC - PubMed
-
- Khan N, Kahl B. Targeting BCL-2 in hematologic malignancies. Targeted Oncol. 2018:257–267. - PubMed
-
- Davids MS. Targeting BCL-2 in B-cell lymphomas. Blood. 2017;130:1081–1088. - PubMed
-
- Davids MS, Roberts AW, Seymour JF, Pagel JM, Kahl BS, Wierda WG, Puvvada S, Kipps TJ, Anderson MA, Salem AH, Dunbar M, Zhu M, Peale F, Ross JA, Gressick L, Desai M, Kim SY, Verdugo M, Humerickhouse RA, Gordon GB, Gerecitano JF. Phase I first-in-human study of venetoclax in patients with relapsed or refractory non-Hodgkin lymphoma. J. Clin. Oncol. 2017;35:826–833. - PMC - PubMed
-
- Tam C, Roberts AW, Anderson M, Dawson S, Hicks R, Burbury K, Turner G, Di Iulio J, Bressel M, Westerman D. Combination ibrutinib (Ibr) and venetoclax (Ven) for the treatment of mantle cell lymphoma (MCL): primary endpoint assessment of the phase 2 AIM study. Hematol Oncol. 2017;35:144–145.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous