

Risk factors for anti-drug antibody formation to infliximab: Secondary analyses of a randomised controlled trial
- PMID: 35411981
- PMCID: PMC9545769
- DOI: 10.1111/joim.13495
Risk factors for anti-drug antibody formation to infliximab: Secondary analyses of a randomised controlled trial
Abstract
Background: Anti-drug antibodies (ADAb) frequently form early in the treatment course of infliximab and other tumour necrosis factor (TNF) inhibitors, leading to treatment failure and adverse events.
Objective: To identify risk factors for ADAb in the early phase of infliximab treatment.
Methods: Patients (n = 410) with immune-mediated inflammatory diseases who initiated infliximab treatment were included in the 38-week Norwegian Drug Monitoring Trial (NOR-DRUM) A and randomised 1:1 to therapeutic drug monitoring (TDM) or standard therapy. Serum levels of infliximab and ADAb were measured at each infusion. Possible risk factors for ADAb formation were assessed using logistic regression, adjusting for potential confounders.
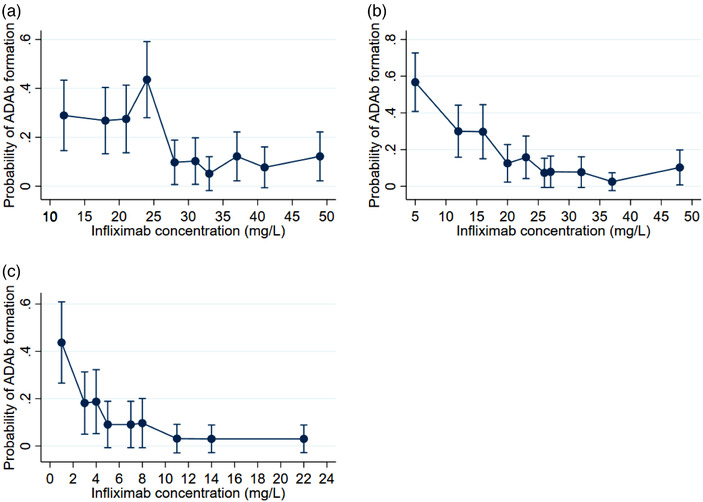
Results: ADAb were detected in 78 (19%) patients. A diagnosis of rheumatoid arthritis (RA) (odds ratio [OR], 1.9 [95% confidence interval [CI] 1.0-3.6]) and lifetime smoking (OR, 2.0 [CI 1.1-3.6]) were baseline risk factors, while baseline use of concomitant immunosuppressors (OR, 0.4 [CI 0.2-0.8]) and a diagnosis of spondyloarthritis (SpA) (OR, 0.4 [CI 0.2-0.8]) reduced the risk of ADAb. Higher disease activity during follow-up (OR, 1.1 [CI 1.0-1.1]) and "drug holidays" of more than 11 weeks (OR, 4.1 [CI 1.2-13.8]) increased the risk of ADAb, whereas higher infliximab doses (OR, 0.1 [CI 0.0-0.3) and higher serum infliximab concentrations (OR, 0.7 [CI 0.6-0.8]) reduced the risk of immunogenicity.
Conclusion: Several risk factors for ADAb formation during early-phase infliximab treatment were identified. This knowledge provides a basis for treatment strategies to mitigate the formation of ADAb and identify patients in whom these measures are of particular importance.
Keywords: autoimmune disease; immunosuppressive treatment.
© 2022 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
Dr. Brun has nothing to disclose. Dr. Goll reports personal fees from AbbVie, personal fees from Pfizer, personal fees from Sandoz, personal fees from Celltrion, personal fees from Lilly, personal fees from UCB, and personal fees from Boehringer Ingelheim outside the submitted work. Dr. Jørgensen reports personal fees from BMS, personal fees from Roche, and Celltrion grants from South‐Eastern Norway Regional Health Authorities. Dr. Sexton has nothing to disclose. Dr. Gehin has nothing to disclose. Dr. Sandanger has nothing to disclose. Dr. Olsen has nothing to disclose. Dr. Klaasen has nothing to disclose. Dr. Warren has nothing to disclose.
Dr. Mørk reports personal fees from Novartis Norge AS, personal fees from LEO Pharma AS, personal fees from ACO Hud Norge AS, personal fees from Cellgene AS, personal fees from Abbvie, and personal fees from Galderma Nordic AB and Eli‐Lilly outside the submitted work.
Dr. Kvien reports grants from the Norwegian Regional Health Authorities (inter‐regional KLINBEFOSK grants) and grants from South‐Eastern Norway Regional Health Authorities during the conduct of the study, grants from AbbVie, grants from Amgen, personal fees from Amgen, grants from BMS, personal fees from Celltrion, personal fees from Egis, personal fees from Evapharma, personal fees from Ewopharma, personal fees from Gilead, personal fees from Hikma, personal fees from Mylan, grants from Novartis, personal fees from Oktal, grants from Pfizer, personal fees from Pfizer, personal fees from Sandoz, personal fees from Sanofi, grants from UCB, and personal fees from UCB outside the submitted work. Dr. Jahnsen has nothing to disclose. Dr. Bolstad reports personal fees from Roche, personal fees from Janssen, and personal fees from Novartis outside the submitted work. Dr. Haavardsholm reports grants from Norwegian Regional Health Authorities (inter‐regional KLINBEFORSK grants) and grants from the South‐Eastern Norway Regional Health Authority during the conduct of the study, personal fees from Pfizer, personal fees from AbbVie, personal fees from Celgene, personal fees from Novartis, personal fees from Janssen, personal fees from Gilead, personal fees from Eli‐Lilly, and personal fees from UCB outside the submitted work. Dr. Syversen reports grants from Norwegian Regional Health Authorities and grants from South‐Eastern Norway Regional Health Authorities during the conduct of the study and personal fees from Thermo Fisher outside the submitted work.
Figures


References
-
- Maini R, St Clair EW, Breedveld F, Furst D, Kalden J, Weisman M, et al. Infliximab (chimeric anti‐tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT study group. Lancet. 1999;354(9194):1932–9. - PubMed
-
- Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462–76. - PubMed
-
- Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, et al. Maintenance infliximab for Crohn's disease: the ACCENT I randomised trial. Lancet 2002;359(9317):1541–9. - PubMed
-
- Chaudhari U, Romano P, Mulcahy LD, Dooley LT, Baker DG, Gottlieb AB. Efficacy and safety of infliximab monotherapy for plaque‐type psoriasis: a randomised trial. Lancet 2001;357(9271):1842–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
