Dosing Regimens of Intravitreal Aflibercept for Diabetic Macular Edema Beyond the First Year: VIOLET, a Prospective Randomized Trial
- PMID: 35412227
- PMCID: PMC9123040
- DOI: 10.1007/s12325-022-02119-z
Dosing Regimens of Intravitreal Aflibercept for Diabetic Macular Edema Beyond the First Year: VIOLET, a Prospective Randomized Trial
Abstract
Introduction: The purpose was to compare two flexible regimens of intravitreal aflibercept (IVT-AFL) with fixed dosing every 8 weeks, beyond the first year of treatment, in patients with diabetic macular edema (DME). VIOLET was a 100-week, randomized, Phase IIIb, non-inferiority study in patients with center-involving DME previously treated with IVT-AFL for ≥ 1 year according to the European label.
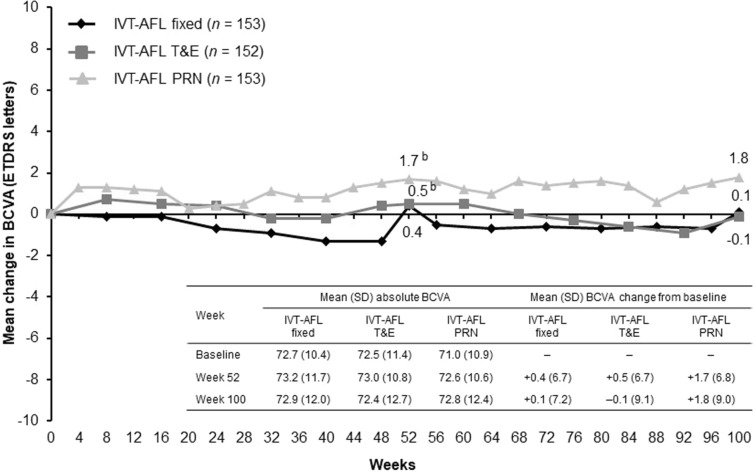
Methods: Patients received an initial dose of IVT-AFL at study baseline and were randomly assigned (1:1:1) to treat-and-extend (T&E), pro re nata (PRN), or fixed regimens. The primary endpoint was mean change in best-corrected visual acuity (BCVA) from baseline (randomization) to Week 52.
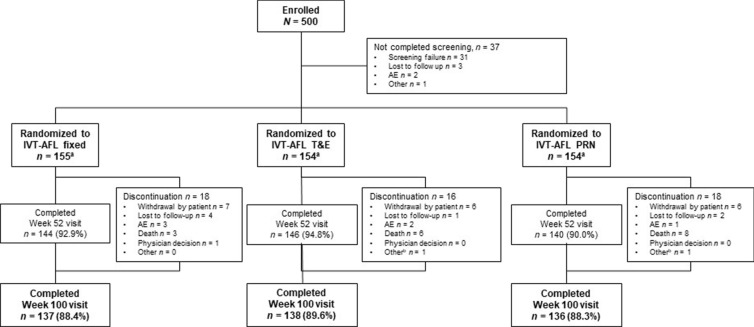
Results: Full analysis set comprised 458 patients (baseline mean BCVA: 72.5, 71.0, and 72.7 letters in the T&E, PRN, and fixed-dose groups, respectively). Patients received a mean (min-max) of 10.0 (2-14; T&E), 11.5 (1-25; PRN), and 12.3 (3-13; fixed) injections over 100 weeks, with 13.3 (4-23), 25.0 (3-29), and 16.1 (5-25) clinic visits, respectively. At Week 52, mean (± standard deviation) BCVA changes from baseline were + 0.5 ± 6.7 (T&E), + 1.7 ± 6.8 (PRN), and + 0.4 ± 6.7 (fixed-dosing) letters (least squares mean difference [95% confidence interval]: T&E 0.01 [- 1.46, 1.47] and PRN 0.95 (- 0.52, 2.42) letters versus fixed dosing; p < 0.0001 for both non-inferiority tests [4-letter margin]). The IVT-AFL safety profile was consistent with previous studies.
Conclusion: The treatment burden associated with intravitreal injections for DME is lowest with T&E regimens, but there are a range of flexible IVT-AFL dosing regimens, allowing physicians to adopt an individualized treatment plan.
Trial registration: ClinicalTrials.gov identifier: NCT02818998.
Keywords: Aflibercept; Diabetic retinopathy; Intravitreal injections; Macular edema; Treatment outcome; Vascular endothelial growth factor.
© 2022. The Author(s).
Figures