

Risk of Adverse Pregnancy Outcomes Among Pregnant Individuals With Gestational Diabetes by Race and Ethnicity in the United States, 2014-2020
- PMID: 35412565
- PMCID: PMC9006108
- DOI: 10.1001/jama.2022.3189
Risk of Adverse Pregnancy Outcomes Among Pregnant Individuals With Gestational Diabetes by Race and Ethnicity in the United States, 2014-2020
Abstract
Importance: Gestational diabetes, which increases the risk of adverse pregnancy outcomes, has been increasing in frequency across all racial and ethnic subgroups in the US.
Objective: To assess whether the frequency of adverse pregnancy outcomes among those in the US with gestational diabetes changed over time and whether the risk of these outcomes differed by maternal race and ethnicity.
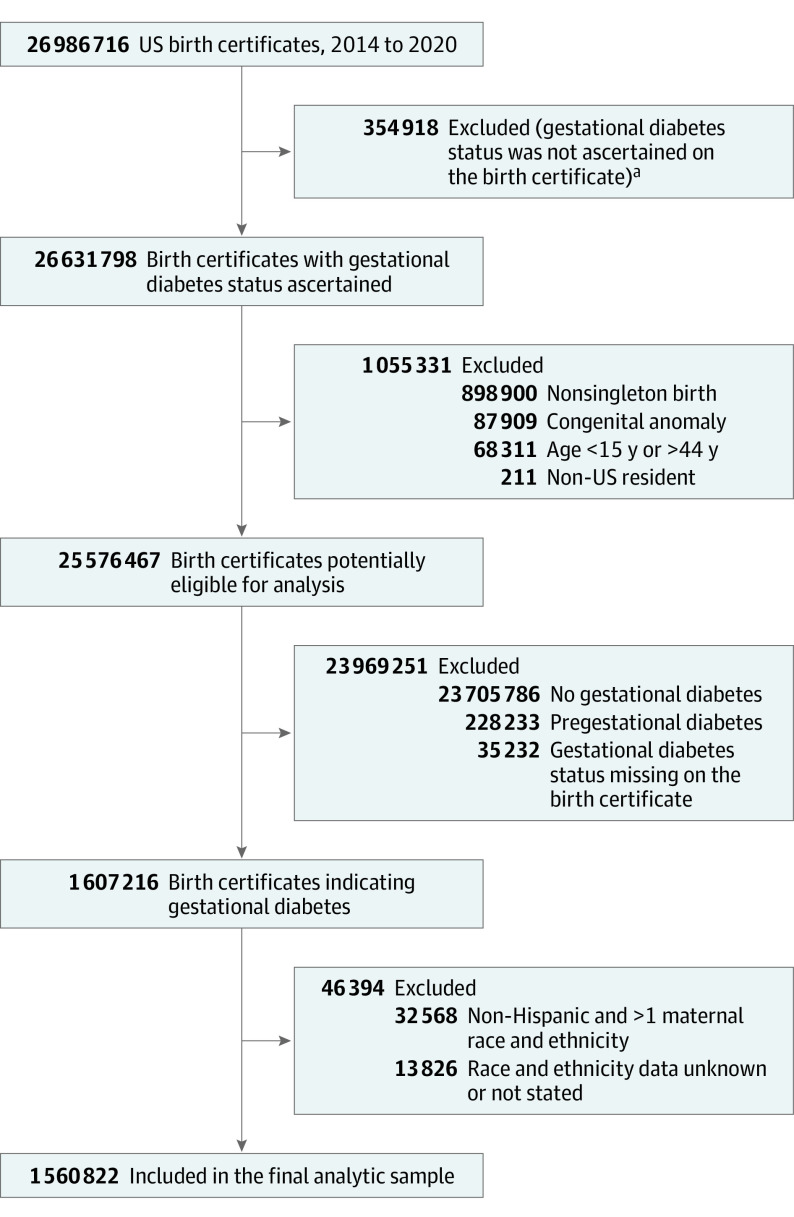
Design, setting, and participants: Exploratory serial, cross-sectional, descriptive study using US National Center for Health Statistics natality data for 1 560 822 individuals with gestational diabetes aged 15 to 44 years with singleton nonanomalous live births from 2014 to 2020 in the US.
Exposures: Year of delivery and race and ethnicity, as reported on the birth certificate, stratified as non-Hispanic American Indian, non-Hispanic Asian/Pacific Islander, non-Hispanic Black, Hispanic/Latina, and non-Hispanic White (reference group).
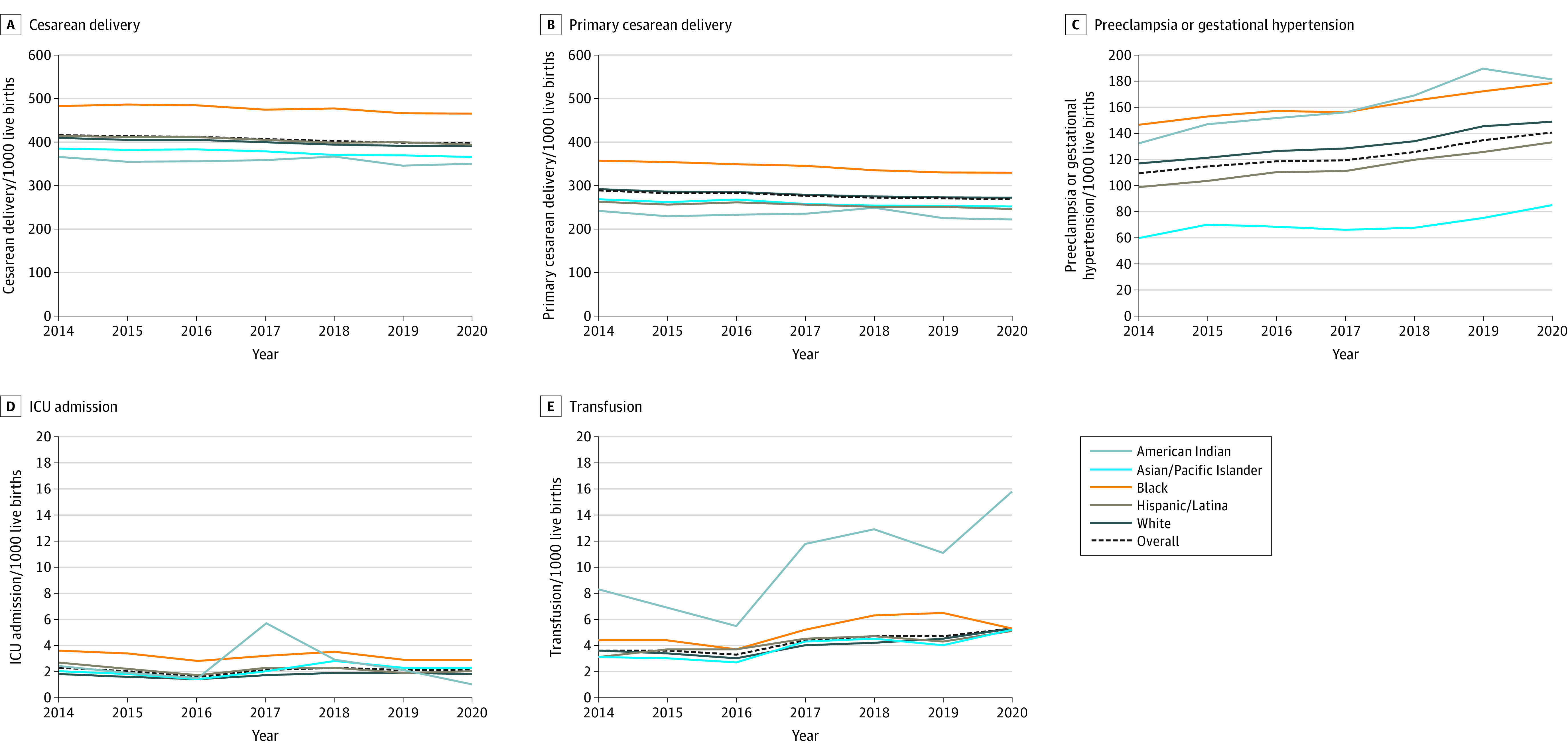
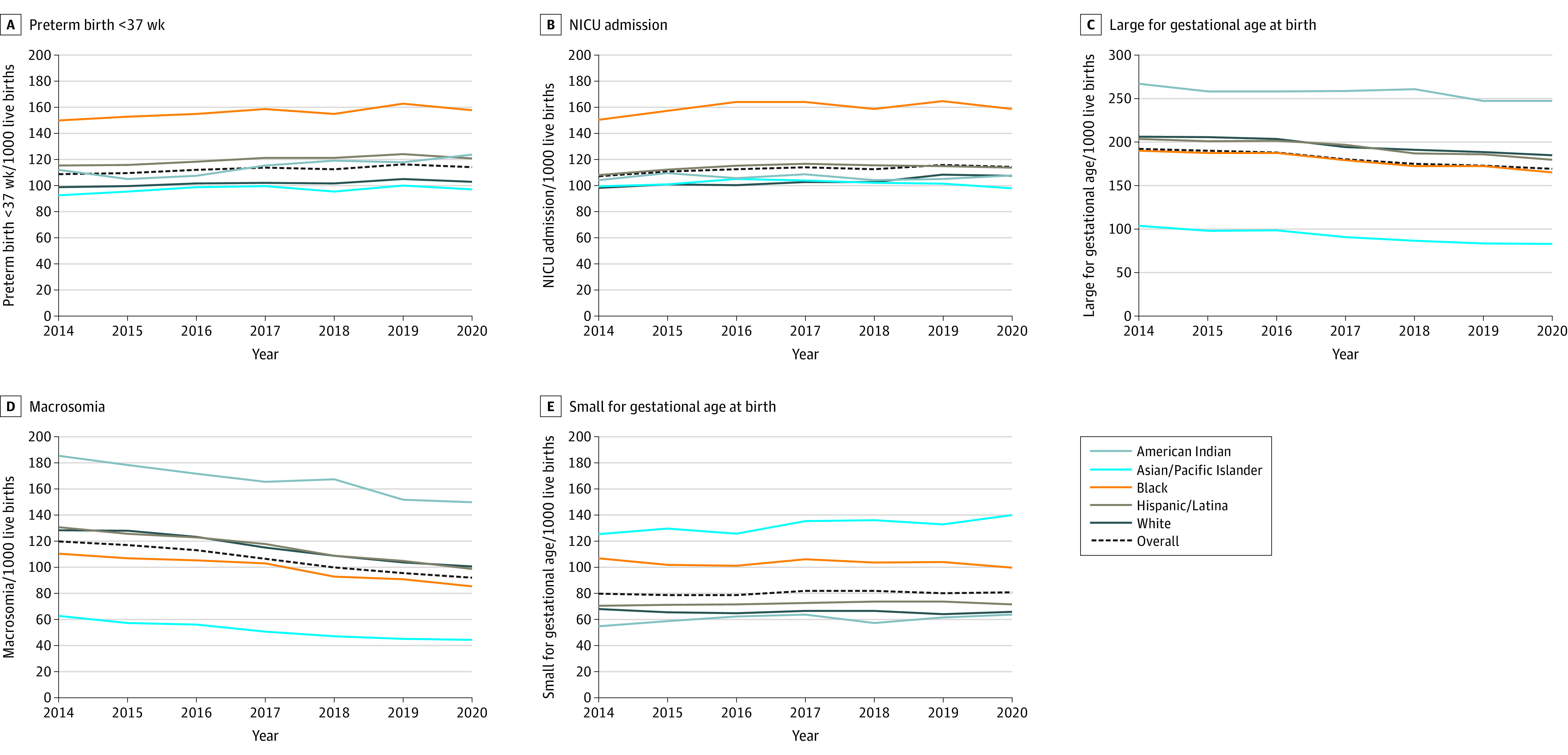
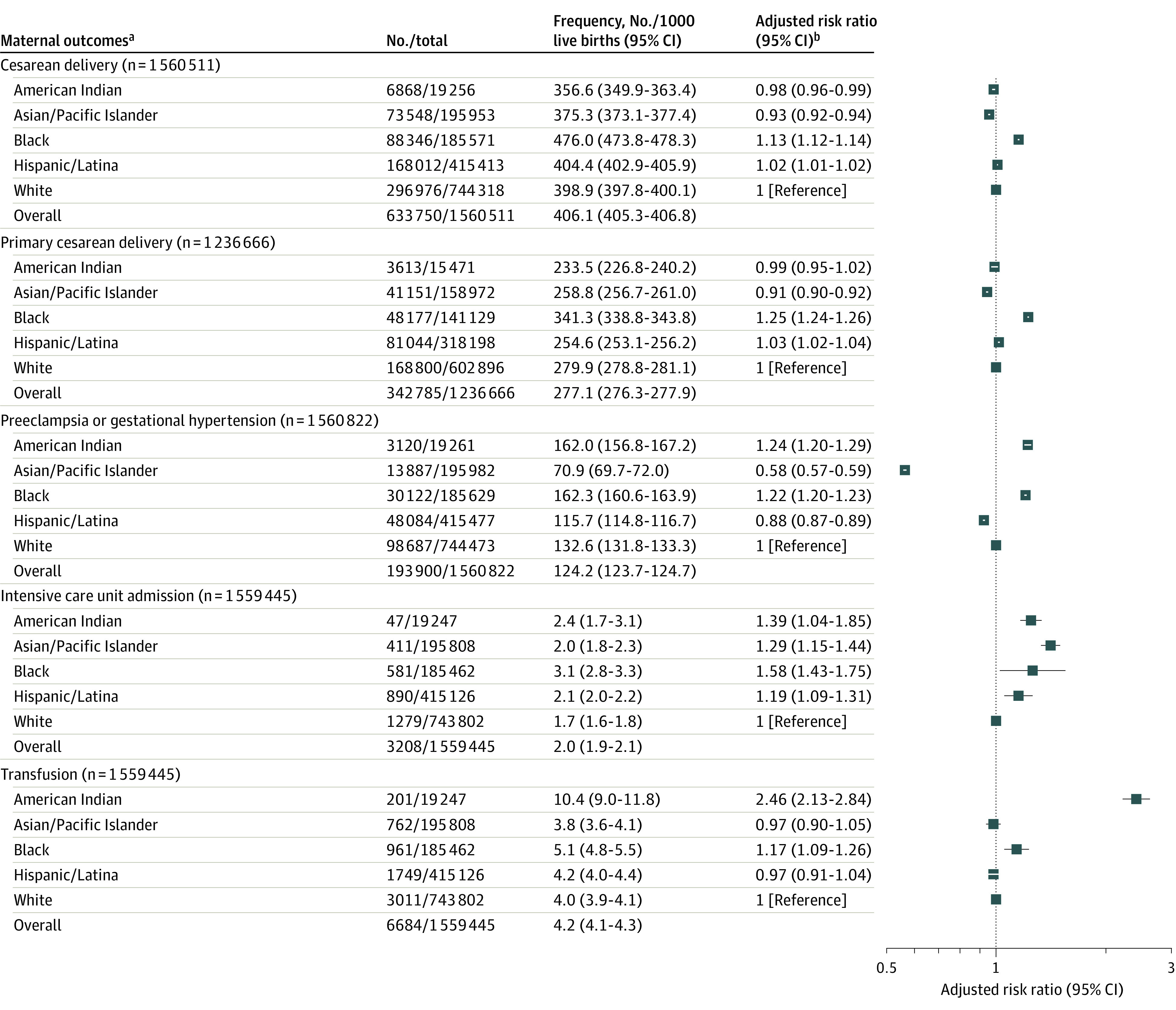
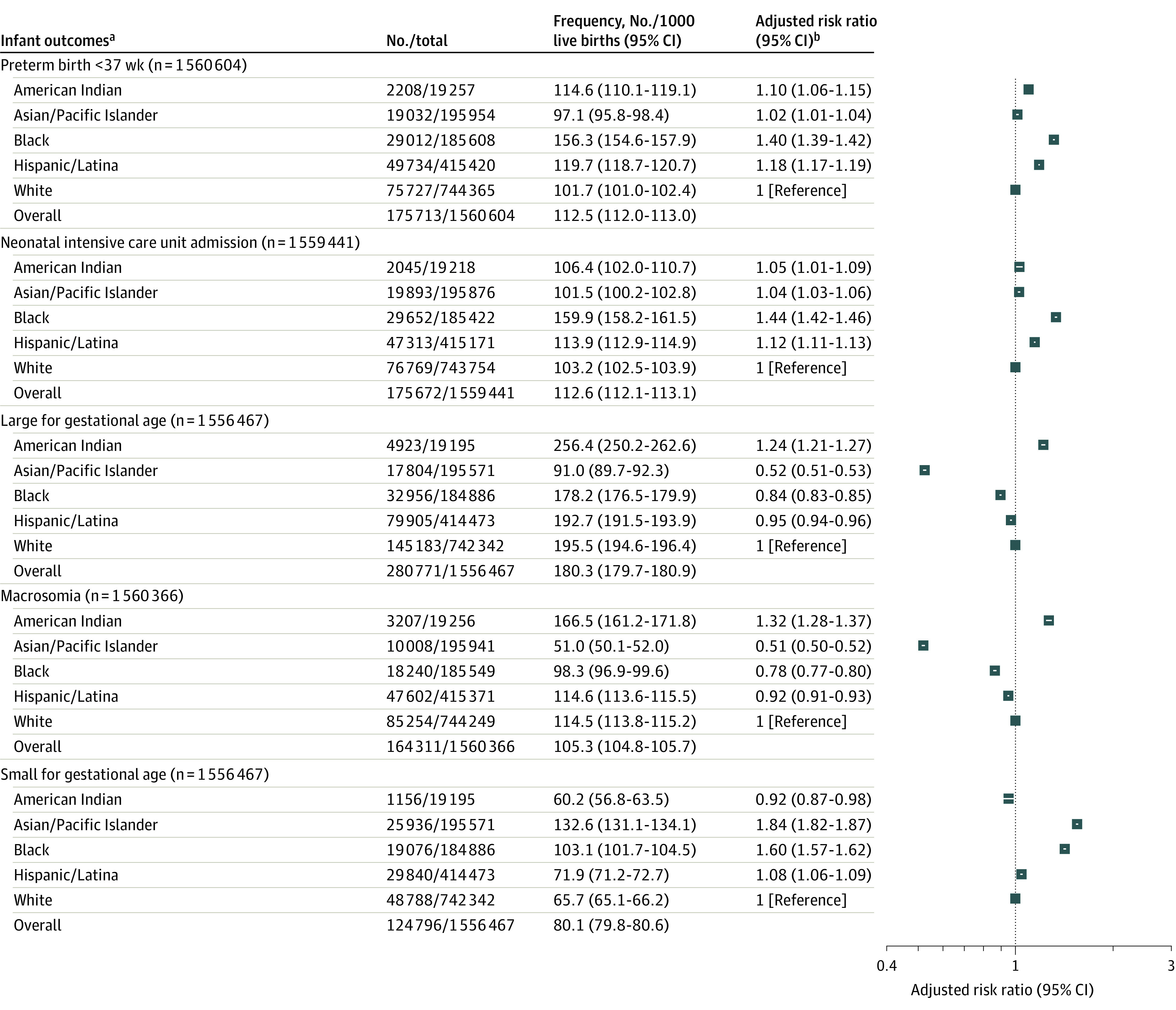
Main outcomes and measures: Maternal outcomes of interest included cesarean delivery, primary cesarean delivery, preeclampsia or gestational hypertension, intensive care unit (ICU) admission, and transfusion; neonatal outcomes included large for gestational age (LGA), macrosomia (>4000 g at birth), small for gestational age (SGA), preterm birth, and neonatal ICU (NICU) admission, as measured by the frequency (per 1000 live births) with estimation of mean annual percentage change (APC), disparity ratios, and adjusted risk ratios.
Results: Of 1 560 822 included pregnant individuals with gestational diabetes (mean [SD] age, 31 [5.5] years), 1% were American Indian, 13% were Asian/Pacific Islander, 12% were Black, 27% were Hispanic/Latina, and 48% were White. From 2014 to 2020, there was a statistically significant increase in the overall frequency (mean APC per year) of preeclampsia or gestational hypertension (4.2% [95% CI, 3.3% to 5.2%]), transfusion (8.0% [95% CI, 3.8% to 12.4%]), preterm birth at less than 37 weeks (0.9% [95% CI, 0.3% to 1.5%]), and NICU admission (1.0% [95% CI, 0.3% to 1.7%]). There was a significant decrease in cesarean delivery (-1.4% [95% CI, -1.7% to -1.1%]), primary cesarean delivery (-1.2% [95% CI, -1.5% to -0.9%]), LGA (-2.3% [95% CI, -2.8% to -1.8%]), and macrosomia (-4.7% [95% CI, -5.3% to -4.0%]). There was no significant change in maternal ICU admission and SGA. In comparison with White individuals, Black individuals were at significantly increased risk of all assessed outcomes, except LGA and macrosomia; American Indian individuals were at significantly increased risk of all assessed outcomes except cesarean delivery and SGA; and Hispanic/Latina and Asian/Pacific Islander individuals were at significantly increased risk of maternal ICU admission, preterm birth, NICU admission, and SGA. Differences in adverse outcomes by race and ethnicity persisted through these years.
Conclusions and relevance: From 2014 through 2020, the frequency of multiple adverse pregnancy outcomes in the US increased among pregnant individuals with gestational diabetes. Differences in adverse outcomes by race and ethnicity persisted.
Conflict of interest statement
Figures
Comment in
-
Risk of Adverse Pregnancy Outcomes Among US Individuals With Gestational Diabetes by Race and Ethnicity.JAMA. 2022 Jul 26;328(4):397. doi: 10.1001/jama.2022.9412. JAMA. 2022. PMID: 35881129 No abstract available.
-
Risk of Adverse Pregnancy Outcomes Among US Individuals With Gestational Diabetes by Race and Ethnicity.JAMA. 2022 Jul 26;328(4):396-397. doi: 10.1001/jama.2022.9409. JAMA. 2022. PMID: 35881130 No abstract available.
References
-
- Landon MB, Spong CY, Thom E, et al. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network . A multicenter, randomized trial of treatment for mild gestational diabetes. N Engl J Med. 2009;361(14):1339-1348. doi: 10.1056/NEJMoa0902430 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
