

Associations Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants and Risk of Coronavirus Disease 2019 (COVID-19) Hospitalization Among Confirmed Cases in Washington State: A Retrospective Cohort Study
- PMID: 35412591
- PMCID: PMC9047245
- DOI: 10.1093/cid/ciac279
Associations Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants and Risk of Coronavirus Disease 2019 (COVID-19) Hospitalization Among Confirmed Cases in Washington State: A Retrospective Cohort Study
Abstract
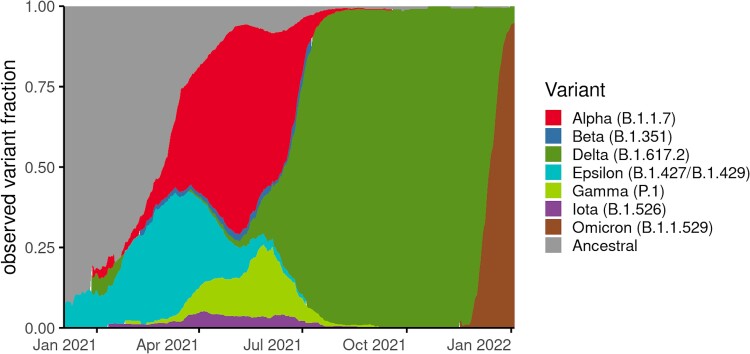
Background: The coronavirus disease 2019 (COVID-19) pandemic is dominated by variant viruses; the resulting impact on disease severity remains unclear. Using a retrospective cohort study, we assessed the hospitalization risk following infection with 7 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants.
Methods: Our study includes individuals with positive SARS-CoV-2 reverse transcription polymerase chain reaction (RT-PCR) in the Washington Disease Reporting System with available viral genome data, from 1 December 2020 to 14 January 2022. The analysis was restricted to cases with specimens collected through sentinel surveillance. Using a Cox proportional hazards model with mixed effects, we estimated hazard ratios (HR) for hospitalization risk following infection with a variant, adjusting for age, sex, calendar week, and vaccination.
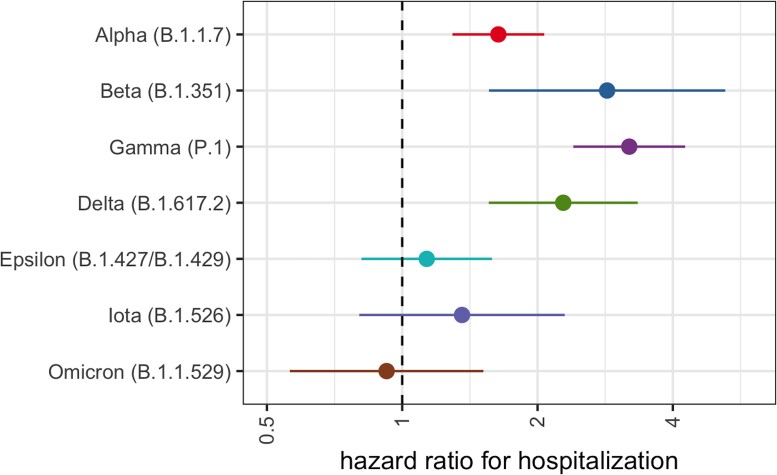
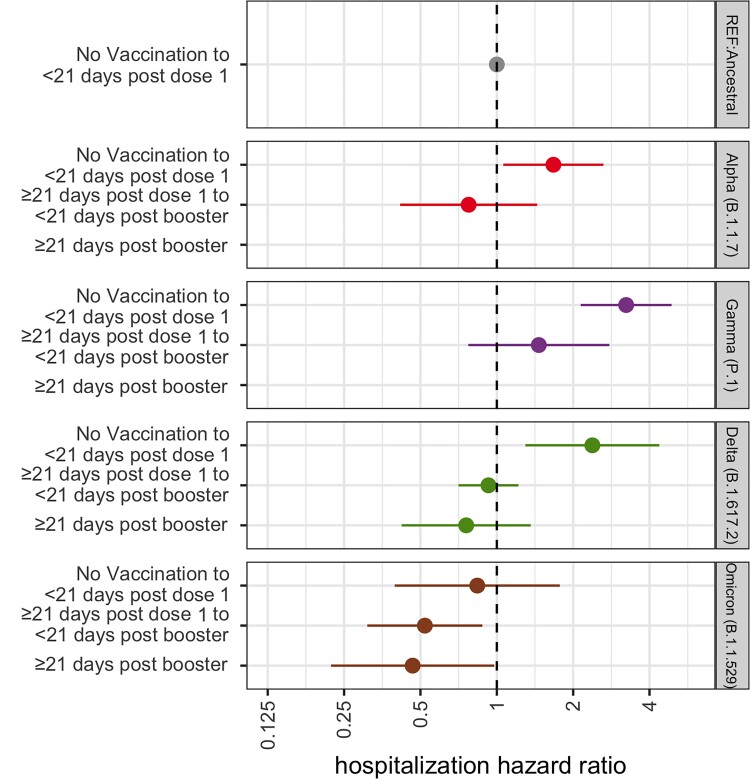
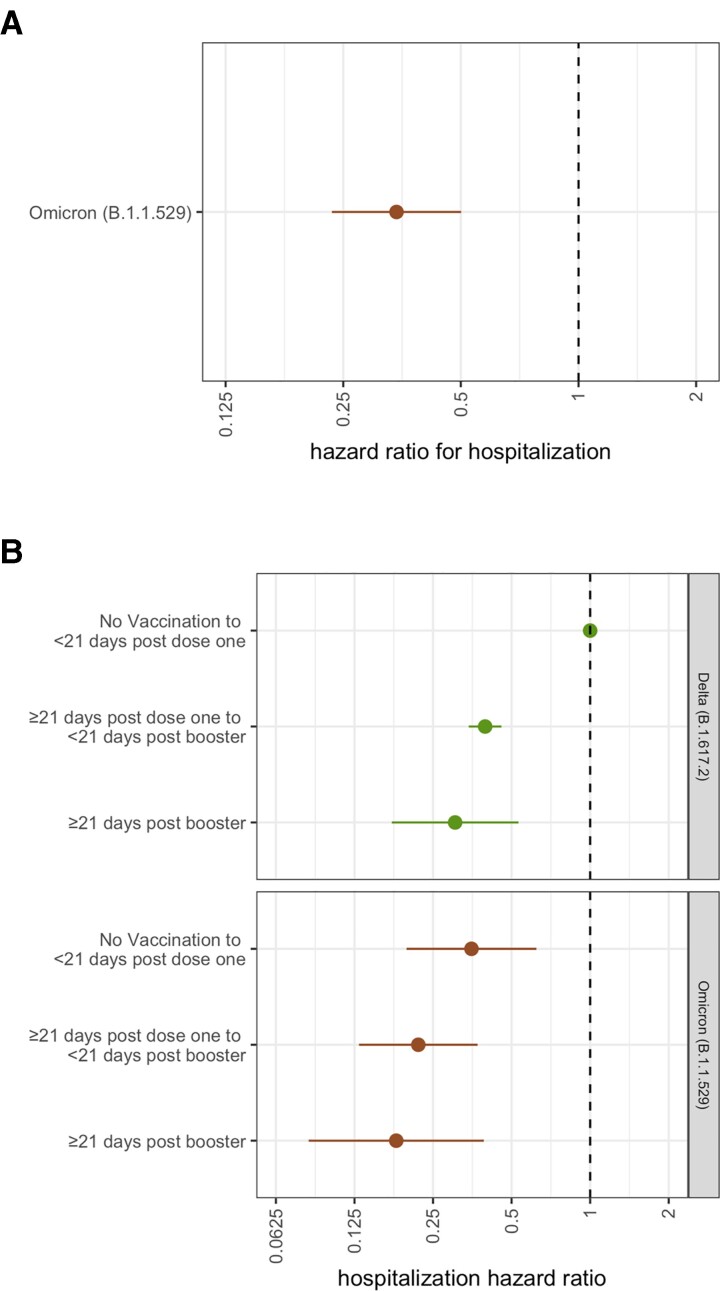
Results: In total, 58 848 cases were sequenced through sentinel surveillance, of which 1705 (2.9%) were hospitalized due to COVID-19. Higher hospitalization risk was found for infections with Gamma (HR 3.20, 95% confidence interval [CI] 2.40-4.26), Beta (HR 2.85, 95% CI 1.56-5.23), Delta (HR 2.28 95% CI 1.56-3.34), or Alpha (HR 1.64, 95% CI 1.29-2.07) compared to infections with ancestral lineages; Omicron (HR 0.92, 95% CI .56-1.52) showed no significant difference in risk. Following Alpha, Gamma, or Delta infection, unvaccinated patients show higher hospitalization risk, while vaccinated patients show no significant difference in risk, both compared to unvaccinated, ancestral lineage cases. Hospitalization risk following Omicron infection is lower with vaccination.
Conclusions: Infection with Alpha, Gamma, or Delta results in a higher hospitalization risk, with vaccination attenuating that risk. Our findings support hospital preparedness, vaccination, and genomic surveillance.
Keywords: COVID-19; SARS-CoV-2; hospitalization; vaccination; variants.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interests. A. L. G. reports central testing lab contract from Abbott and research funding from Merck and Gilead. K. A. became an employee of Biobot Analytics after the initial manuscript submission. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Update of
-
Associations between SARS-CoV-2 variants and risk of COVID-19 hospitalization among confirmed cases in Washington State: a retrospective cohort study.medRxiv [Preprint]. 2022 Feb 16:2021.09.29.21264272. doi: 10.1101/2021.09.29.21264272. medRxiv. 2022. Update in: Clin Infect Dis. 2022 Aug 24;75(1):e536-e544. doi: 10.1093/cid/ciac279. PMID: 34729567 Free PMC article. Updated. Preprint.
References
-
- CDC . Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention. 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html. Accessed 3 August 2021.
-
- Washington State Department of Health . First cases of U.K. COVID-19 strain found in Washington state. 2021. Available at: https://www.doh.wa.gov/Newsroom/Articles/ID/2581/First-case-of-UK-COVID-.... Accessed 3 August 2021.
-
- Washington State Department of Health . SARS-CoV-2 Sequencing and Variants in Washington State. 2021. Available at: https://doh.wa.gov/sites/default/files/2022-02/420-316-SequencingAndVari....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
