

Association of Subcutaneous or Intravenous Administration of Casirivimab and Imdevimab Monoclonal Antibodies With Clinical Outcomes in Adults With COVID-19
- PMID: 35412625
- PMCID: PMC9006104
- DOI: 10.1001/jamanetworkopen.2022.6920
Association of Subcutaneous or Intravenous Administration of Casirivimab and Imdevimab Monoclonal Antibodies With Clinical Outcomes in Adults With COVID-19
Abstract
Importance: Monoclonal antibody (mAb) treatment decreases hospitalization and death in high-risk outpatients with mild to moderate COVID-19; however, only intravenous administration has been evaluated in randomized clinical trials of treatment. Subcutaneous administration may expand outpatient treatment capacity and qualified staff available to administer treatment, but the association with patient outcomes is understudied.
Objectives: To evaluate whether subcutaneous casirivimab and imdevimab treatment is associated with reduced 28-day hospitalization and death compared with nontreatment among mAb-eligible patients and whether subcutaneous casirivimab and imdevimab treatment is clinically and statistically similar to intravenous casirivimab and imdevimab treatment.
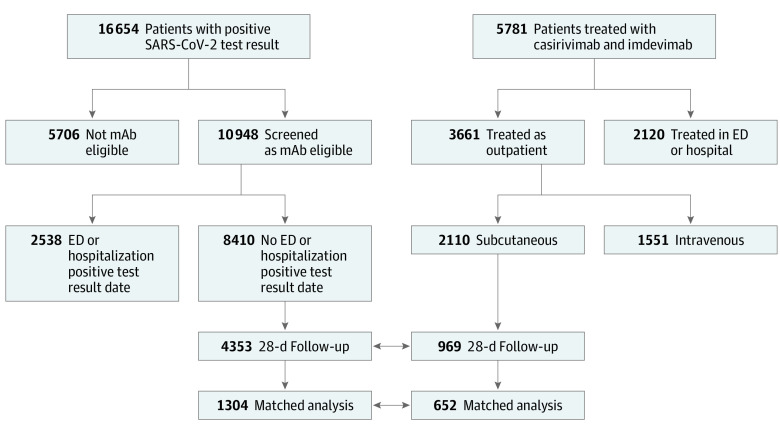
Design, setting, and participants: This prospective cohort study evaluated high-risk outpatients in a learning health system in the US with mild to moderate COVID-19 symptoms from July 14 to October 26, 2021, who were eligible for mAb treatment under emergency use authorization. A nontreated control group of eligible patients was also studied.
Exposures: Subcutaneous injection or intravenous administration of the combined single dose of 600 mg of casirivimab and 600 mg of imdevimab.
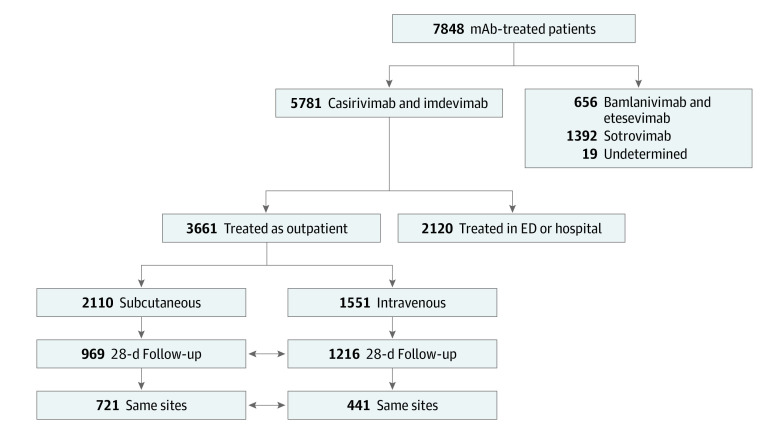
Main outcomes and measures: The primary outcome was the 28-day adjusted risk ratio or adjusted risk difference for hospitalization or death. Secondary outcomes included 28-day adjusted risk ratios and differences in hospitalization, death, a composite end point of emergency department admission and hospitalization, and rates of adverse events. Among 1959 matched adults with mild to moderate COVID-19, 969 patients (mean [SD] age, 53.8 [16.7] years; 547 women [56.4%]) who received casirivimab and imdevimab subcutaneously had a 28-day rate of hospitalization or death of 3.4% (22 of 653 patients) compared with 7.0% (92 of 1306 patients) in nontreated controls (risk ratio, 0.48; 95% CI, 0.30-0.80; P = .002). Among 2185 patients treated with subcutaneous (n = 969) or intravenous (n = 1216; mean [SD] age, 54.3 [16.6] years; 672 women [54.4%]) casirivimab and imdevimab, the 28-day rate of hospitalization or death was 2.8% vs 1.7%, which resulted in an adjusted risk difference of 1.5% (95% CI, -0.6% to 3.5%; P = .16). Among all infusion patients, there was no difference in intensive care unit admission (adjusted risk difference, 0.7%; 95% CI, -3.5% to 5.0%) or need for mechanical ventilation (adjusted risk difference, 0.2%; 95% CI, -5.8% to 5.5%).
Conclusions and relevance: In this cohort study of high-risk outpatients with mild to moderate COVID-19 symptoms, subcutaneously administered casirivimab and imdevimab was associated with reduced hospitalization and death when compared with no treatment. These results provide preliminary evidence of potential expanded use of subcutaneous mAb treatment, particularly in areas that are facing treatment capacity and/or staffing shortages.
Conflict of interest statement
Figures
References
-
- Weinreich DM, Sivapalasingam S, Norton T, et al. . REGEN-COV antibody cocktail clinical outcomes study in Covid-19 outpatients. medRxiv. 2021:2021.05.19.21257469. doi:10.1101/2021.05.19.21257469 - DOI
-
- US Food and Drug Administration . Fact sheet for health care providers emergency use authorization (EUA) of REGEN-COVTM. November 21, 2020. Accessed November 23, 2021. https://www.regeneron.com/downloads/treatment-covid19-eua-fact-sheet-for...
-
- GOV.UK . Patient information leaflet for Ronapreve. November 19, 2021. Accessed November 23, 2021. https://www.gov.uk/government/publications/regulatory-approval-of-ronapr...
-
- Huang DT, McCreary EK, Bariola JR, et al. . The UPMC OPTIMISE-C19 (optimizing treatment and impact of monoclonal antibodies through evaluation for COVID-19) trial: a structured summary of a study protocol for an open-label, pragmatic, comparative effectiveness platform trial with response-adaptive randomization. Trials. 2021;22(1):363. doi:10.1186/s13063-021-05316-3 - DOI - PMC - PubMed
