

Independent risk factors for myasthenic crisis and disease exacerbation in a retrospective cohort of myasthenia gravis patients
- PMID: 35413850
- PMCID: PMC9005160
- DOI: 10.1186/s12974-022-02448-4
Independent risk factors for myasthenic crisis and disease exacerbation in a retrospective cohort of myasthenia gravis patients
Abstract
Background: Myasthenic crisis (MC) and disease exacerbation in myasthenia gravis (MG) are associated with significant lethality and continue to impose a high disease burden on affected patients. Therefore, we sought to determine potential predictors for MC and exacerbation as well as to identify factors affecting outcome.
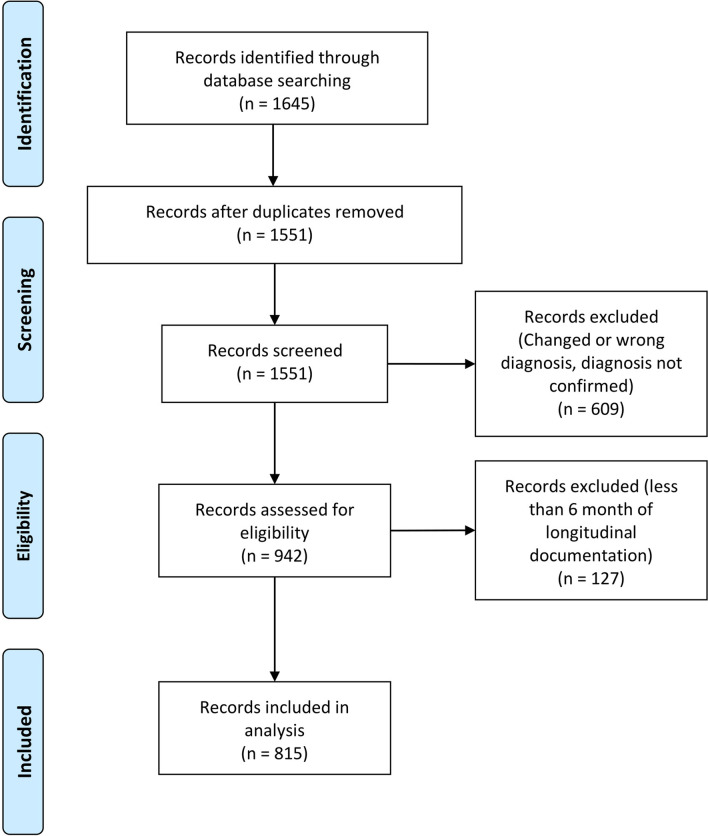
Methods: We examined a retrospective, observational cohort study of patients diagnosed with MG between 2000 and 2021 with a mean follow-up of 62.6 months after diagnosis from eight tertiary hospitals in Germany. A multivariate Cox regression model with follow-up duration as the time variable was used to determine independent risk factors for MC and disease exacerbation.
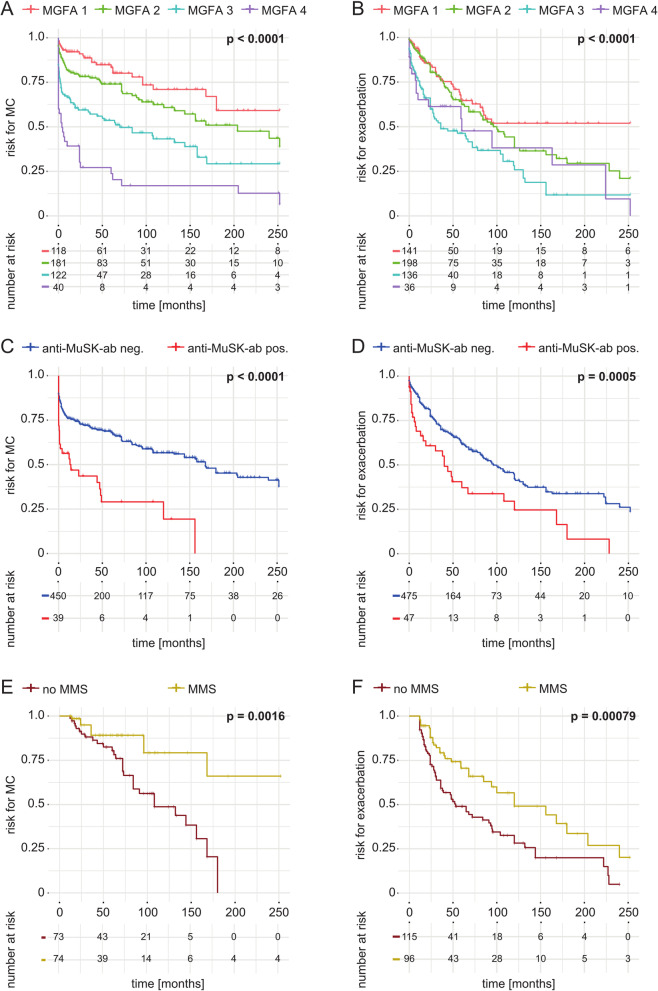
Results: 815 patients diagnosed with MG according to national guidelines were included. Disease severity at diagnosis (quantitative MG score or Myasthenia Gravis Foundation of America class), the presence of thymoma and anti-muscle specific tyrosine kinase-antibodies were independent predictors of MC or disease exacerbation. Patients with minimal manifestation status 12 months after diagnosis had a lower risk of MC and disease exacerbation than those without. The timespan between diagnosis and the start of immunosuppressive therapy did not affect risk. Patients with a worse outcome of MC were older, had higher MGFA class before MC and at admission, and had lower vital capacity before and at admission. The number of comorbidities, requirement for intubation, prolonged mechanical ventilation, and MC triggered by infection were associated with worse outcome. No differences between outcomes were observed comparing treatments with IVIG (intravenous immunoglobulin) vs. plasma exchange vs. IVIG together with plasma exchange.
Conclusions: MC and disease exacerbations inflict a substantial burden of disease on MG patients. Disease severity at diagnosis and antibody status predicted the occurrence of MC and disease exacerbation. Intensified monitoring with emphasis on the prevention of infectious complications could be of value to prevent uncontrolled disease in MG patients.
Keywords: Disease exacerbation; Myasthenia gravis; Myasthenic crisis; Predictors; Risk factors.
© 2022. The Author(s).
Conflict of interest statement
Dr. Nelke reports no disclosures. Dr. Stascheit received speaking Honoria from Biogen and Alexion. Cand. med. Eckert reports no disclosures. Dr. Pawlitzki received speaker honoraria and travel/accommodation/meeting expenses from Novartis. Dr. Mergenthaler is on the Advisory Board of HealthNextGen Inc. and has equity interest in the company. His research is funded by the Bundesministerium für Bildung und Forschung (BMBF), the European Union, the Else Kröner-Fresenius Stiftung, the Volkswagen Stiftung, and the Einstein Foundation Berlin. Dr Schroeter reports no disclosures. Dr. Arat reports no disclosures. Dr. Özturk reports no disclosures. Prof. Föll reports no disclosures. Prof. Schreiber reports no disclosures. Prof. Vielhaber reports no disclosures. Dr. Gassa reports no disclosures. Dr. Stetefeld reports not disclosures. Prof. Schroeter reports no disclosures. Dr. Berger received travel grants and/or training expenses from Bayer Vital GmbH, IpsenPharma GmbH, Norvartis, Biogen GmbH and Genzyme, as well as lecture fees from Ipsen Pharma GmbH, Alexion Pharma GmbH, Merck, Sanofi Genzyme and Roche. Dr. Totzeck reports no disclosures. Dr. Hagenacker received speaker and advisory board honoraria from Alexion, Biogen and Roche. Prof. Meuth receives honoraria for lecturing, and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Bundesinstitut für Risikobewertung (BfR), Deutsche Forschungsgemeinschaft (DFG), Deutsche Multiple Sklerose Gesellschaft (DMSG), Else Kröner Fresenius Foundation, Gemeinsamer Bundesausschuss (G-BA), German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and Alexion, Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, HERZ Burgdorf, Merck Serono, Novartis, ONO Pharma, Roche, and Teva. Prof. Wiendl receives honoraria for acting as a member of Scientific Advisory Boards, Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG, and Sanofi-Aventis as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche Ltd., Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, TEVA, and WebMD Global. Prof. Wiendl is acting as a paid consultant for Abbvie, Actelion, Biogen, IGES, Johnson & Johnson, Novartis, Roche, Sanofi-Aventis, and the Swiss Multiple Sclerosis Society. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Fresenius Foundation, the European Union, Hertie Foundation, NRW Ministry of Education and Research, Interdisciplinary Center for Clinical Studies (IZKF) Muenster and RE Children’s Foundation, Biogen, GlaxoSmithKline GmbH, Roche Pharma AG, Sanofi-Genzyme. Prof. Meisel received speaker honoraria from Alexion, argnx, GRIFOLS and Hormosan. He received honoraria from Alexion, argnx, UCB, Janssen and Vitaccess for consulting services and financial research support from Octapharma and Alexion. Andreas Meisel is chairman of the medical advisory board of the German Myasthenia Gravis Society. Dr. Ruck reports grants from German Ministry of Education, Science, Research and Technology, grants and personal fees from Sanofi-Genzyme and Alexion; personal fees from Biogen, Roche and Teva; personal fees and nonfinancial support from Merck Serono, outside the submitted work.
Figures
References
-
- Lacomis D. Myasthenic crisis. 2005. 10.1385/Neurocrit. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
