

Evaluating quality of care at the end of life and setting best practice performance standards: a population-based observational study using linked routinely collected administrative databases
- PMID: 35413862
- PMCID: PMC9003976
- DOI: 10.1186/s12904-022-00927-2
Evaluating quality of care at the end of life and setting best practice performance standards: a population-based observational study using linked routinely collected administrative databases
Abstract
Background: A high percentage of people dying at home, and a low percentage of people being admitted to hospital and dying there are regarded as indicators of appropriate care at the end of life. However, performance standards for these quality indicators are often lacking, which makes it difficult to state whether an indicator score falls between the ranges of good or poor quality care. The aim of this study was to assess quality indicators concerning place of death and hospital care utilization in people with diseases relevant for palliative care, and to establish best practice performance standards based on indicator scores in 31 regions in the Netherlands.
Methods: A retrospective nationwide population-based observational study was conducted, using routinely collected administrative data concerning persons who died in 2017 in the Netherlands with underlying causes relevant for palliative care (N = 109,707). Data from four registries were linked for analysis. Scores on eight quality indicators concerning place of death and hospital care utilization were calculated, and compared across 31 healthcare insurance regions to establish relative benchmarks.
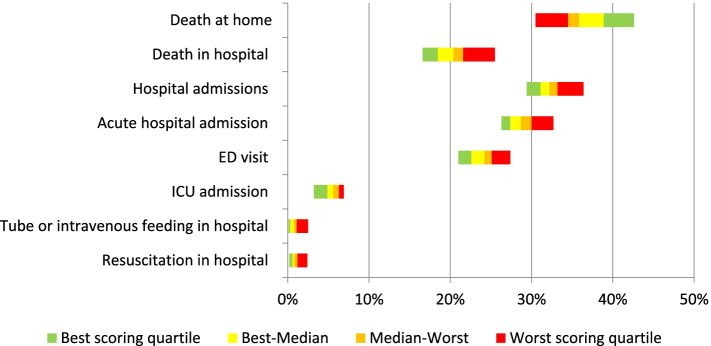
Results: On average, 36.4% of the study population died at home (range between regions 30.5%-42.6%) and 20.4% in hospital (range 16.6%-25.5%). Roughly half of the population who received hospital care at any time in the last year of life were found to (also) receive hospital care in the last month of life. In the last month, 32.0% of the study population were admitted to hospital (range 29.4-36.4%), 5.3% to an Intensive Care Unit (range 3.2-6.9%) and 23.9% visited an Emergency Department (range 21.0-27.4%). In the same time period, less than 1% of the study population was resuscitated in hospital or received tube or intravenous feeding in hospital.
Conclusions: The variation between regions points towards opportunities for practice improvement. The best practice performance standards as set in this study serve as ambitious but attainable targets for those regions that currently do not meet the standards. Policymakers, healthcare providers and researchers can use the suggested performance standards to further analyze causes of variance between regions and develop and test interventions that can improve practice.
Keywords: Benchmarking; End-of-life care; Hospital care; Performance standards; Place of death; Quality indicators; Routinely collected health data.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Gomes B, Higginson IJ, Calanzani N, Cohen J, Deliens L, Daveson BA, et al. Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, the Netherlands. Portugal and Spain Ann Oncol. 2012;23:2006–2015. doi: 10.1093/annonc/mdr602. - DOI - PubMed
-
- Koekoek B. Regie over de plaats van sterven. Een kwantitatieve en kwalitatieve verkenning. (Managing place of death. A quantitative and qualitative exploration) Utrecht: Universiteit Utrecht; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
