

Distinct molecular and immune hallmarks of inflammatory arthritis induced by immune checkpoint inhibitors for cancer therapy
- PMID: 35413951
- PMCID: PMC9005525
- DOI: 10.1038/s41467-022-29539-3
Distinct molecular and immune hallmarks of inflammatory arthritis induced by immune checkpoint inhibitors for cancer therapy
Erratum in
-
Author Correction: Distinct molecular and immune hallmarks of inflammatory arthritis induced by immune checkpoint inhibitors for cancer therapy.Nat Commun. 2024 Jul 4;15(1):5621. doi: 10.1038/s41467-024-49733-9. Nat Commun. 2024. PMID: 38965214 Free PMC article. No abstract available.
Abstract
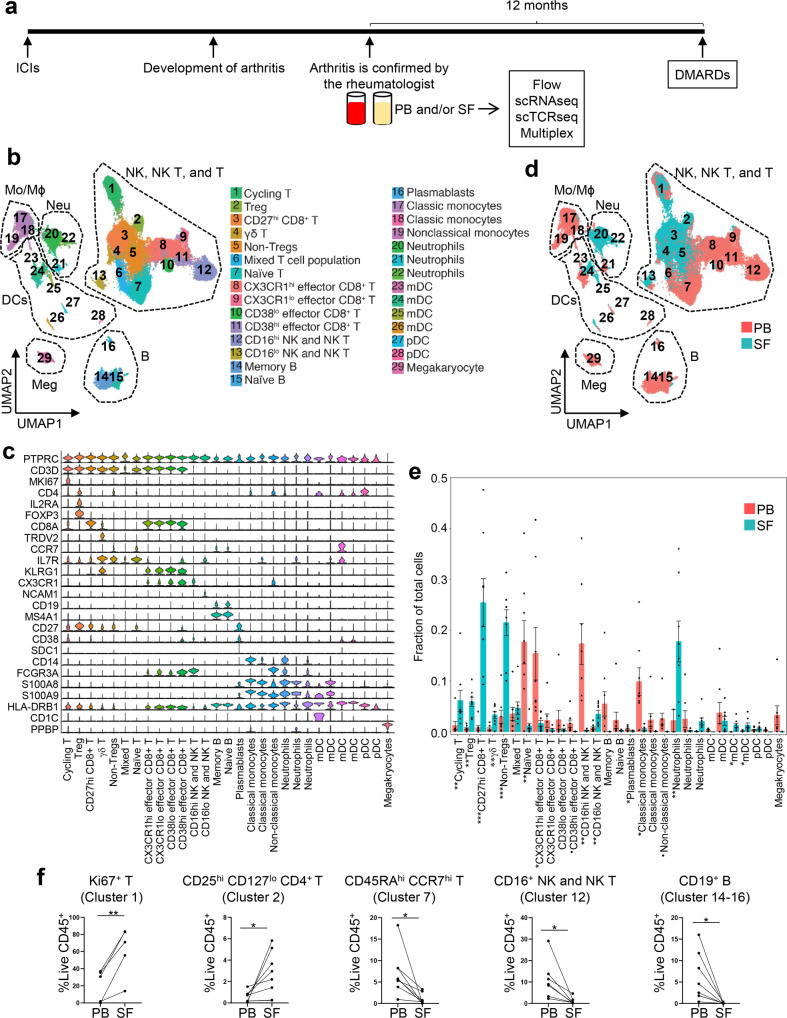
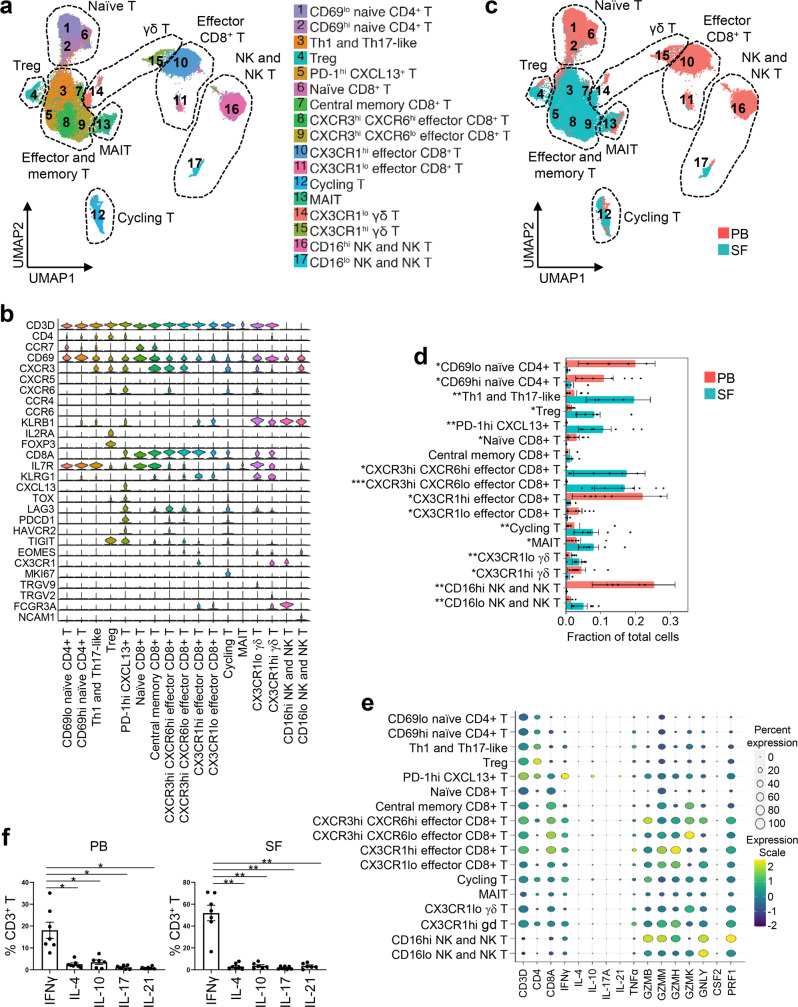
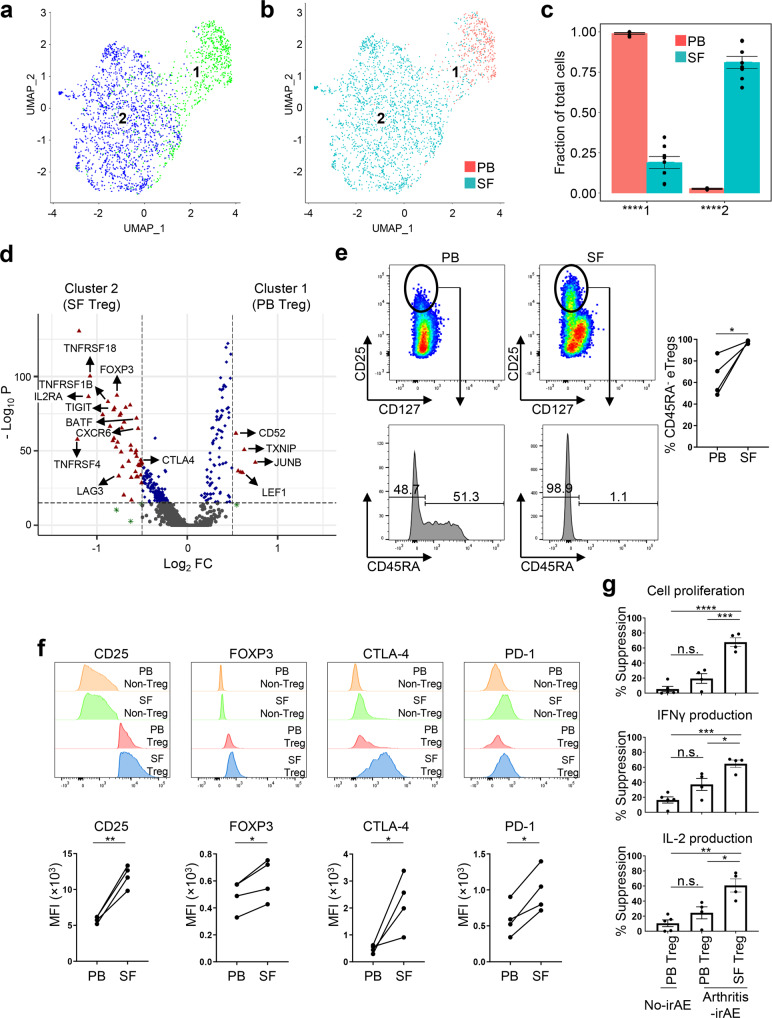
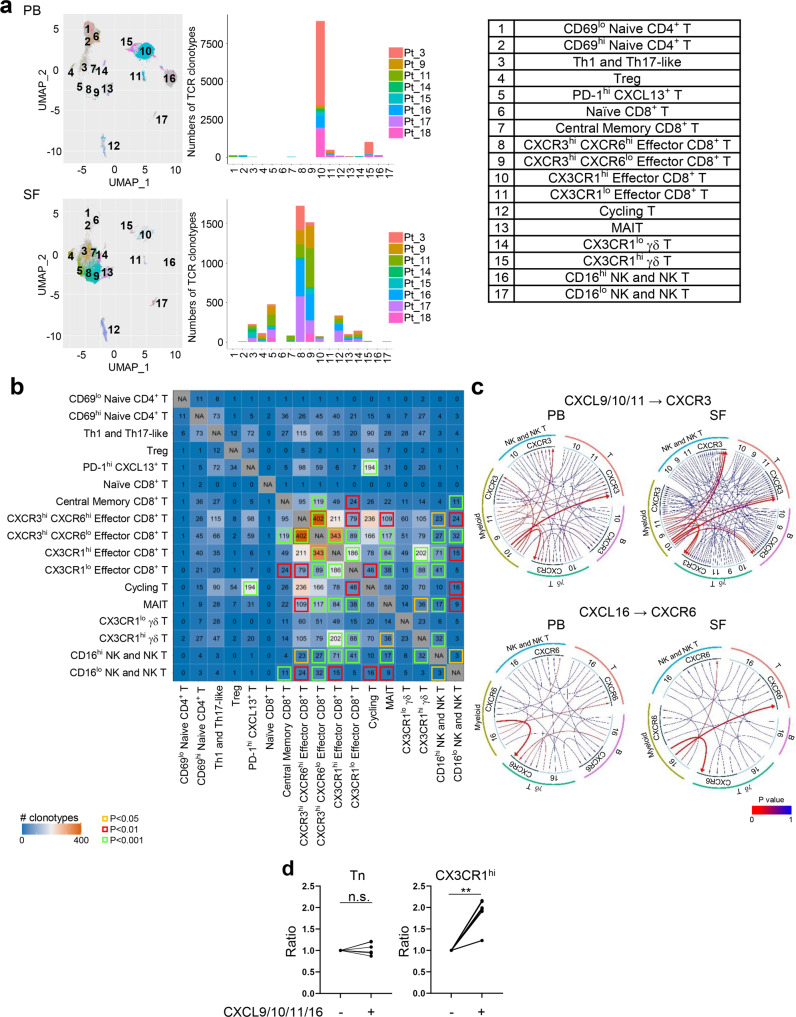
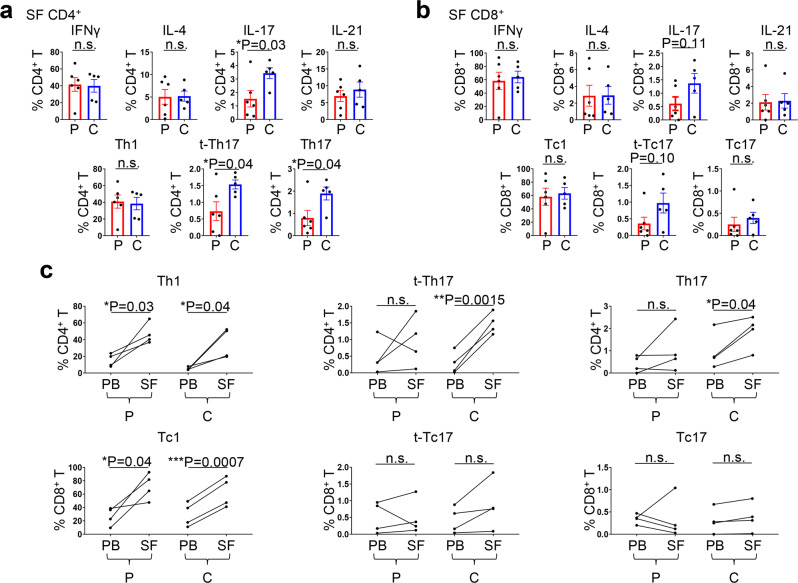
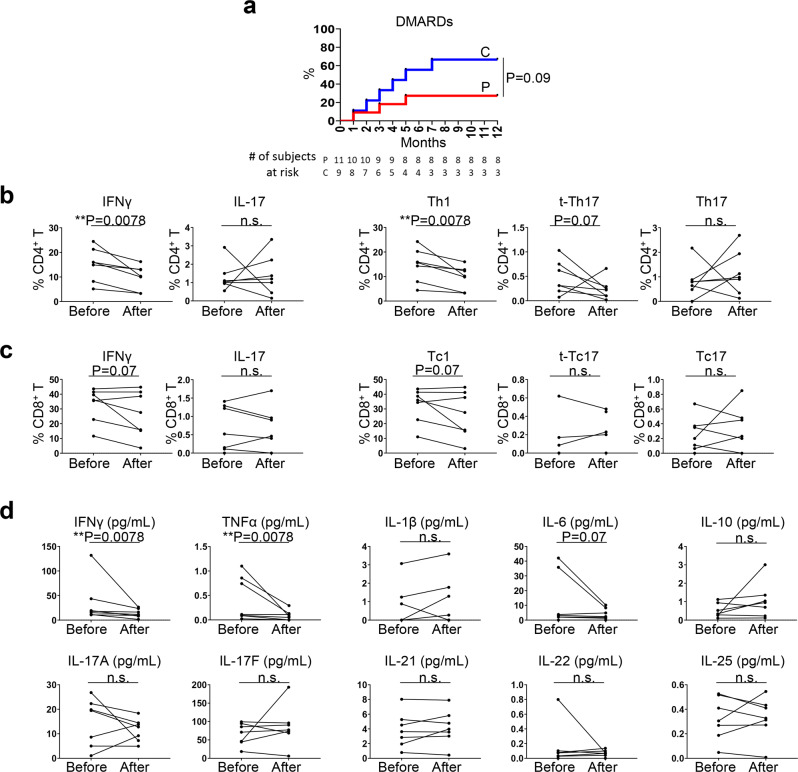
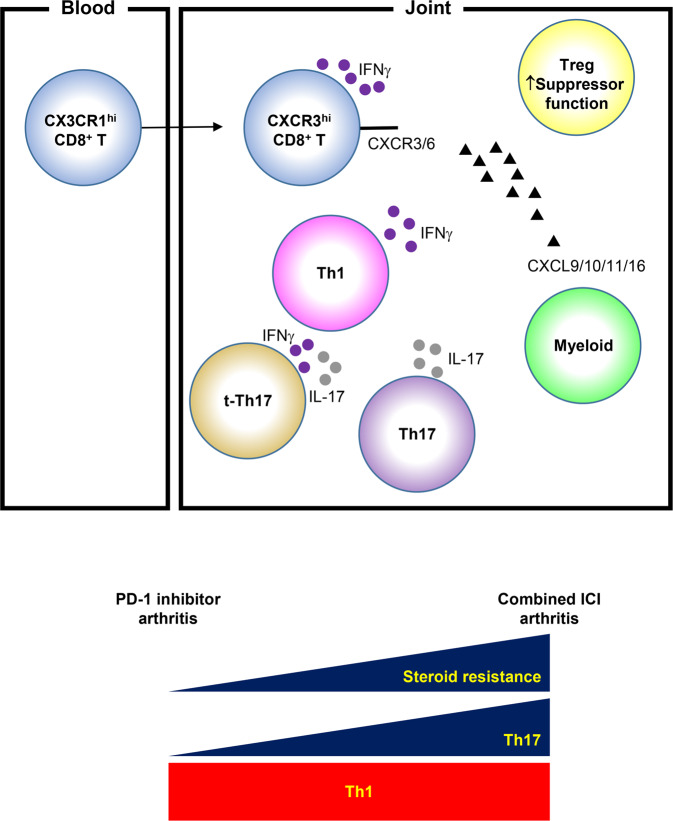
Immune checkpoint inhibitors are associated with immune-related adverse events (irAEs), including arthritis (arthritis-irAE). Management of arthritis-irAE is challenging because immunomodulatory therapy for arthritis should not impede antitumor immunity. Understanding of the mechanisms of arthritis-irAE is critical to overcome this challenge, but the pathophysiology remains unknown. Here, we comprehensively analyze peripheral blood and/or synovial fluid samples from 20 patients with arthritis-irAE, and unmask a prominent Th1-CD8+ T cell axis in both blood and inflamed joints. CX3CR1hi CD8+ T cells in blood and CXCR3hi CD8+ T cells in synovial fluid, the most clonally expanded T cells, significantly share TCR repertoires. The migration of blood CX3CR1hi CD8+ T cells into joints is possibly mediated by CXCL9/10/11/16 expressed by myeloid cells. Furthermore, arthritis after combined CTLA-4 and PD-1 inhibitor therapy preferentially has enhanced Th17 and transient Th1/Th17 cell signatures. Our data provide insights into the mechanisms, predictive biomarkers, and therapeutic targets for arthritis-irAE.
© 2022. The Author(s).
Conflict of interest statement
M.S.-A. has served as a consultant for Gilead, Avenue Therapeutics, ChemoCentryx, Pfizer, Eli Lilly and Bristol Myers Squibb. N.A.-W. has received honoraria for serving on a scientific advisory board for ChemoCentryx and served as a consultant for ChemoCentryx. S.S.N. has received personal fees from Kite, a Gilead Company, Merck, Bristol Myers Squibb, Novartis, Celgene, Pfizer, Allogene Therapeutics, Sellas Life Sciences, Cell Medica/Kuur/Athenex, Incyte, Precision Biosciences, Legend Biotech, Adicet Bio, Calibr, Unum Therapeutics, Bluebird Bio, and Sana Biotechnology; research support from Kite, a Gilead Company, Bristol Myers Squibb, Merck, Poseida, Cellectis, Celgene, Karus Therapeutics, Unum Therapeutics, Allogene Therapeutics, Precision Biosciences, Acerta, and Adicet Bio; royalties from Takeda Pharmaceuticals; and has intellectual property related to cell therapy. M.T.C. has received honoraria for serve on a Scientific Advisory Board for Astellas, Eisai, EMD Serono, Exelixis, Genentech, Pfizer, Seattle Genetics, served as a consultant for ApricityHealth, Exelixis, Pfizer, non-branded educational programs supported by Bristol Myers Squibb, Exelixis, Merck, Pfizer, Roche, and research funding for clinical trials from ApricityHealth, AstraZeneca, EMD Serono/Pfizer, Exelixis, and Janssen. D.L.G. declares advisory board work for Janssen, AstraZeneca, GlaxoSmithKline and Sanofi. D.L.G. receives research grant funding from AstraZeneca, Janssen, Astellas, Ribon Therapeutics, NGM Therapeutics and Takeda. M.A. declares advisory board work for GlaxoSmithKline, Shattuck Lab, Bristol Myers Squibb, AstraZeneca. M.A. has received speaker fees from AstraZeneca, and Nektar Therapeutics. M.A. received research funding from Genentech, Nektar Therapeutics, Merck, GlaxoSmithKline, Novartis, Jounce Therapeutics, Bristol Myers Squibb, Eli Lilly, Adaptimmune, and Shattuck Lab. S.N.W. received research grants to the institution from AstraZeneca, Clovis Oncology, GSK/Tesaro, Roche/Genentech, Novartis, Cotinga Pharmaceuticals, Bayer, Bio-Path, and ArQule, and received consulting fees from AstraZeneca, Clovis Oncology, GSK/Tesaro, Roche/Genentech, Novartis, Merck, Pfizer, Eisai, Zentalis, Circulogene, and Agenus. A.N. received research grants to the institution from NCI, EMD Serono, MedImmune, Healios Onc. Nutrition, Atterocor/Millendo, Amplimmune, ARMO BioSciences, Karyopharm Therapeutics, Incyte, Novartis, Regeneron, Merck, Bristol- Myers Squibb, Pfizer, CytomX Therapeutics, Neon Therapeutics, Calithera Biosciences, TopAlliance Biosciences, Eli Lilly, Kymab, PsiOxus, Arcus Biosciences, NeoImmuneTech, ImmuneOncia, Surface Oncology, Monopteros Therapeutics, BioNTech SE, Seven & Eight Biopharma, and SOTIO Biotech AG. M.A.D. has been a consultant to Roche/Genentech, Array, Pfizer, Novartis, BMS, GSK, Sanofi-Aventis, Vaccinex, Apexigen, Eisai, and ABM Therapeutics, and he has been the PI of research grants to MD Anderson by Roche/Genentech, GSK, Sanofi-Aventis, Merck, Myriad, and Oncothyreon. T.C. has received speakers’ fees from the Society for Immunotherapy of Cancer, Bristol Myers Squibb, Roche, Medscape Oncology and PeerView Institute for Medical Education; reports consulting/advisory role fees from MedImmune, AstraZeneca, Bristol Myers Squibb, Merck & Co., Genentech, Arrowhead Pharmaceuticals and EMD Serono; reports institutional clinical research funding from Boehringer Ingelheim, MedImmune, AstraZeneca, EMD Serono, and Bristol Myers Squibb. The remaining authors declare no competing interests.
Figures
References
-
- Subedi, A., Strauss, J. & Gupta, S. Erosive deforming inflammatory arthritis in a patient with cervical adenocarcinoma. JAMA Oncol.5,1628–1629 (2019). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
