

Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: a systematic review
- PMID: 35414491
- PMCID: PMC8994568
- DOI: 10.1016/j.jphys.2022.03.011
Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: a systematic review
Abstract
Question: How effective and safe is telerehabilitation for people with COVID-19 and post-COVID-19 conditions?
Design: Systematic review of randomised trials.
Participants: People with COVID-19 and post-COVID-19 conditions.
Intervention: Any type of telerehabilitation.
Outcome measures: Satisfaction, quality of life, adverse events, adherence to telerehabilitation, dyspnoea, functional performance, readmissions, mortality, pulmonary function and level of independence.
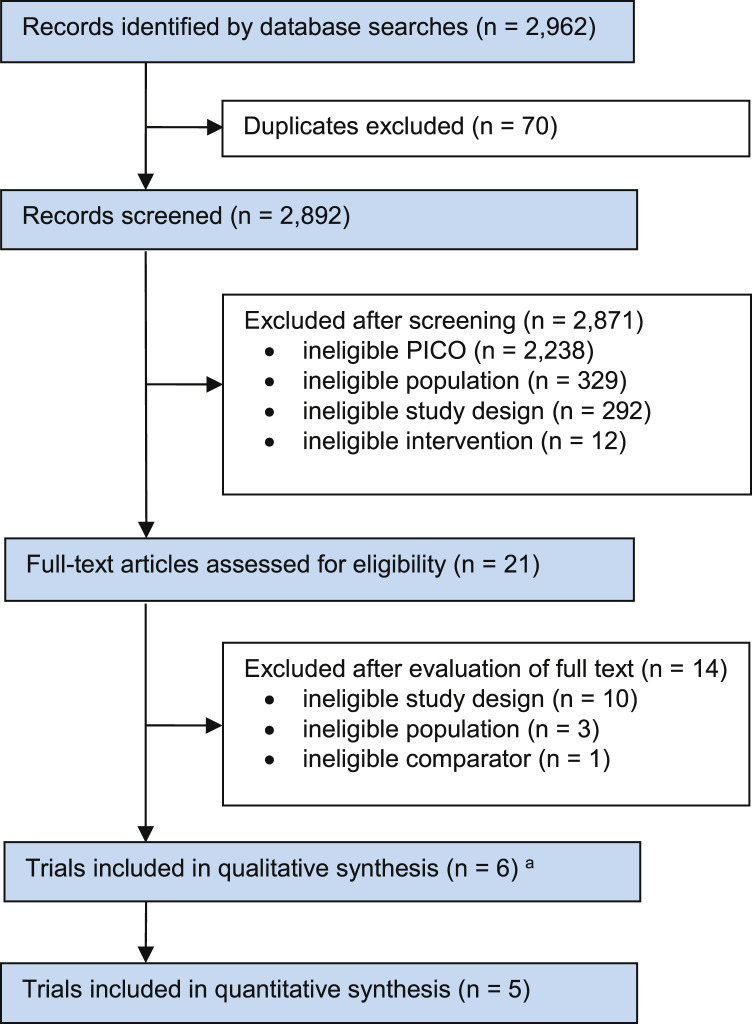
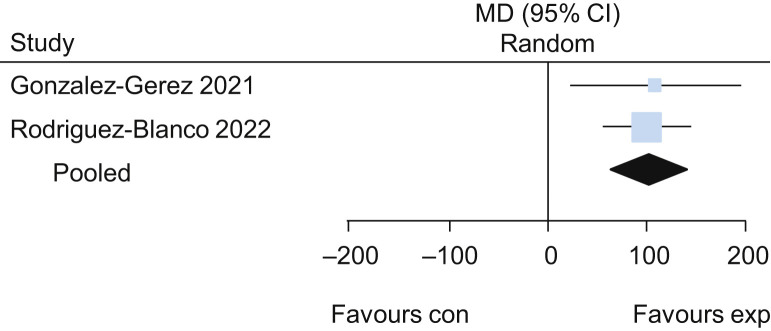
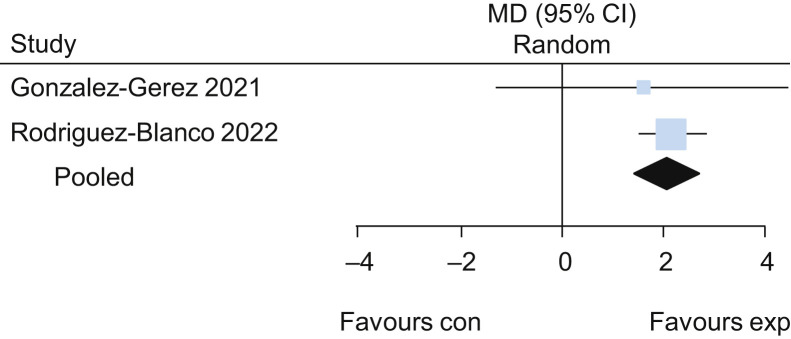
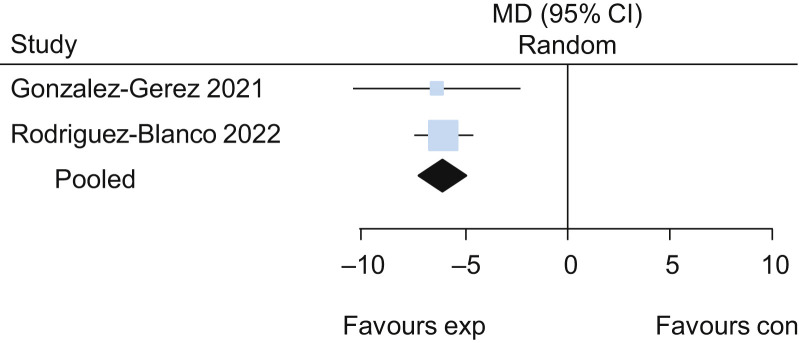
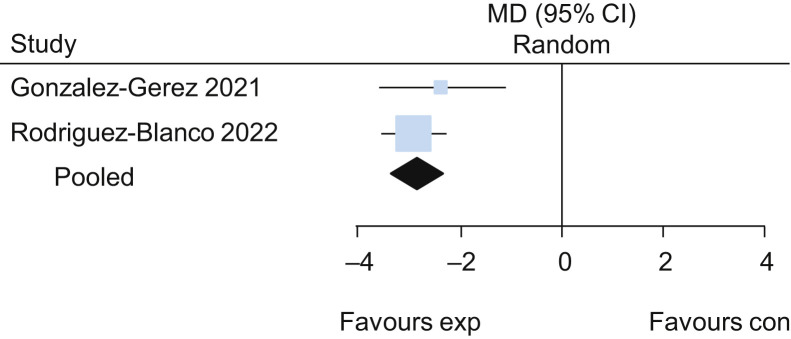
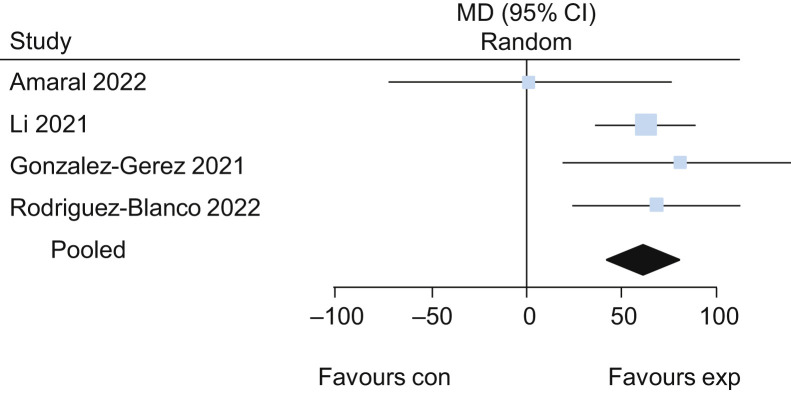
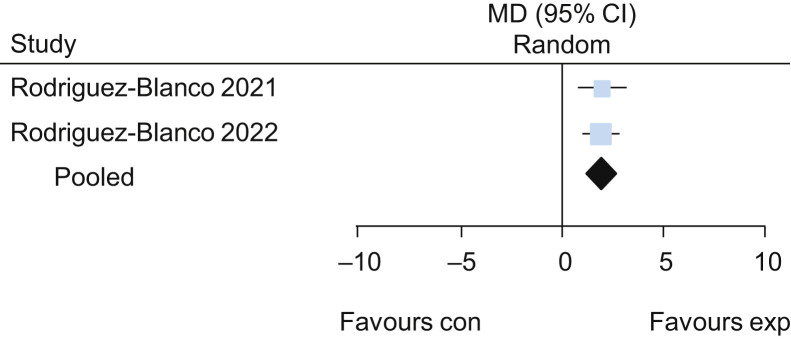
Results: Database searches retrieved 2,962 records, of which six trials with 323 participants were included in the review. Breathing exercises delivered via telerehabilitation improved 6-minute walk distance (MD 101 m, 95% CI 61 to 141; two studies), 30-second sit-to-stand test performance (MD 2.2 repetitions, 95% CI 1.5 to 2.8; two studies), Multidimensional Dyspnoea-12 questionnaire scores (MD -6, 95% CI -7 to -5; two studies) and perceived effort on the 0-to-10 Borg scale (MD -2.8, 95% CI -3.3 to -2.3; two studies), with low certainty of evidence. Exercise delivered via telerehabilitation improved 6-minute walk distance (MD 62 m, 95% CI 42 to 82, four studies), 30-second sit-to-stand test performance (MD 2.0 repetitions, 95% CI 1.3 to 2.7; two studies) and Multidimensional Dyspnoea-12 scores (MD -1.8, 95% CI -2.5 to -1.1; one study), with low certainty of evidence. Adverse events were almost all mild or moderate and occurred with similar frequency in the telerehabilitation group (median 0 per participant, IQR 0 to 2.75) as in the control group (median 0 per participant, IQR 0 to 2); Hodges-Lehmann median difference 0 (95% CI 0 to 0), with low certainty of evidence.
Conclusion: Telerehabilitation may improve functional capacity, dyspnoea, performance and physical components of quality of life and does not substantially increase adverse events.
Registration: PROSPERO CRD42021271049.
Keywords: COVID-19; Patient safety; Physical therapy; Systematic review; Telerehabilitation.
Copyright © 2022 Australian Physiotherapy Association. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int
Websites
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
