

Cardiac Amyloidosis Treatment
- PMID: 35414852
- PMCID: PMC8932359
- DOI: 10.14797/mdcvj.1050
Cardiac Amyloidosis Treatment
Abstract
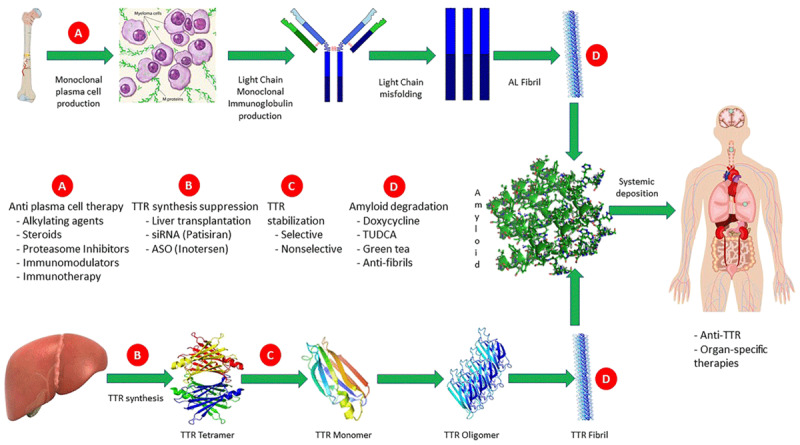
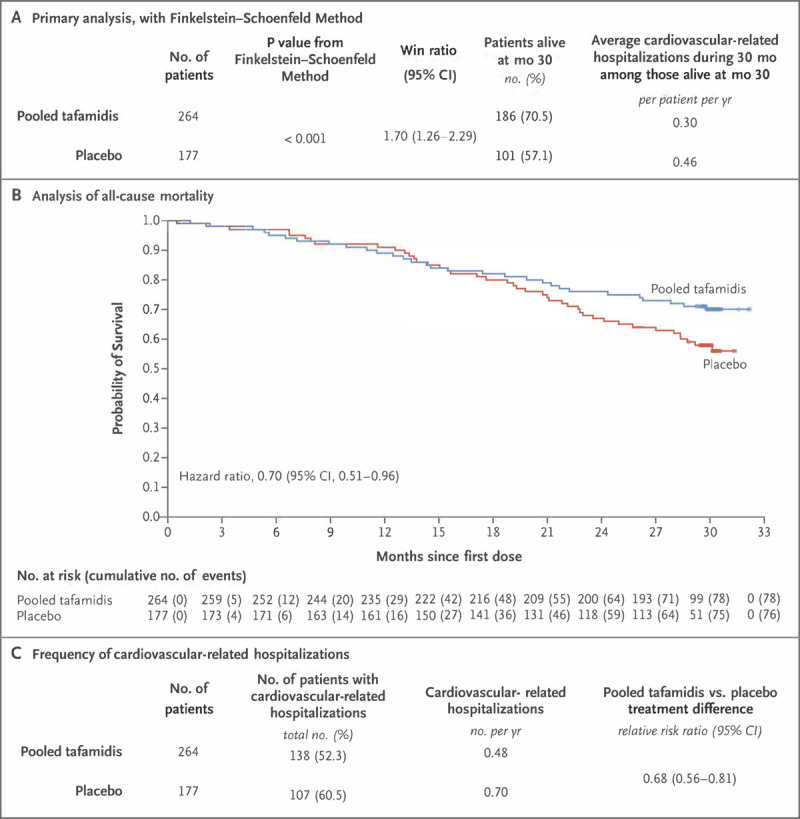
Cardiac amyloidosis (CA) is a restrictive cardiomyopathy with a traditionally poor prognosis. Until recently, CA treatment options were limited and consisted predominantly of managing symptoms and disease-related complications. However, the last decade has seen significant advances in disease-modifying therapies, increased awareness of CA, and improved diagnostic methods resulting in earlier diagnoses. In this review, we provide an overview of current and experimental treatments for the predominant types of CA: transthyretin cardiac amyloidosis (ATTR-CA) and immunoglobulin light chain (AL)-mediated CA (AL-CA). The mainstay of AL-CA treatment is proteasome inhibitor-based chemotherapy with daratumumab and, when feasible, autologous stem cell transplantation. For ATTR-CA, the stabilizer tafamidis is the only US Food and Drug Administration (FDA)-approved treatment. However, promising novel therapies on the horizon target various points in the ATTR-CA amyloidogenic cascade. These include transthyretin gene (TTR) silencing agents to prevent TTR formation, TTR tetramer stabilization and inhibition of oligomer aggregation to prevent fibril formation, anti-TTR fiber antibodies, and amyloid degradation. For end-stage CA, advanced interventions may need to be considered, including heart, heart-kidney, and, for hereditary ATTR-CA, heart-liver transplantation. Despite the evolution of treatment options, CA management remains complex due to patient frailty and therapeutic side effects or intolerance with advanced cardiac disease. This is particularly relevant for those with AL-CA, when active teamwork between the hematologist-oncologist and the cardiologist is critical for treatment success. Often, referral to an expert center is necessary for timely diagnosis, initiation of treatment, and participation in clinical trials.
Keywords: amyloidosis treatment; autologous stem cell transplantation; cardiac amyloidosis; daratumumab; inotersen; light chain amyloidosis; monoclonal light chains; patisiran; tafamidis; transthyretin amyloidosis.
Copyright: © 2022 The Author(s).
Conflict of interest statement
Jignesh Patel is a consultant for Pfizer, Alnylam, Akcea, and BridgeBio. Lily Stern has no competing interests to declare.
Figures
References
-
- Palladini G, Dispenzieri A, Gertz MA, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. 2012. Dec 20;30(36):4541-9. doi: 10.1200/JCO.2011.37.7614 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
