

Clinical Clues and Diagnostic Workup of Cardiac Amyloidosis
- PMID: 35414856
- PMCID: PMC8932349
- DOI: 10.14797/mdcvj.1061
Clinical Clues and Diagnostic Workup of Cardiac Amyloidosis
Abstract
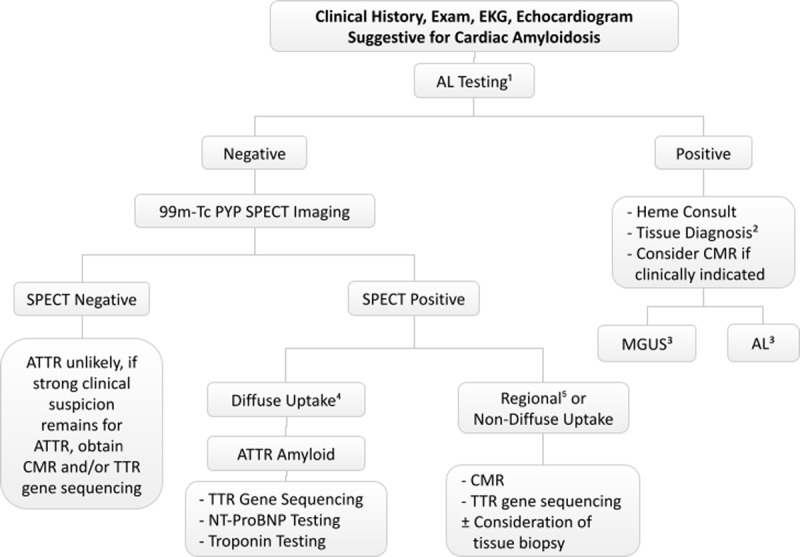
Cardiac amyloidosis is increasingly recognized as an underlying cause of left ventricular wall thickening, heart failure, and arrhythmia with variable clinical presentation. Due to the subtle cardiac findings in early transthyretin cardiac amyloidosis and the availability of therapies that can modify but not reverse the disease progression, early recognition is vital. In light chain amyloidosis, timely diagnosis and treatment can significantly improve survival. In this manuscript, we review the clinical, imaging, and electrocardiographic clues that should raise suspicion for cardiac amyloidosis and provide a simplified diagnostic workup algorithm that ensures an accurate diagnosis. The evolution of the noninvasive diagnosis of cardiac amyloidosis has significantly influenced our understanding of disease prevalence, presentations, and outcomes. However, clinical recognition of clues and red flags remains the most important factor in advancing the care of patients with cardiac amyloidosis.
Keywords: aortic stenosis; bone scintigraphy; cardiac amyloidosis; cardiac magnetic resonance imaging; endomyocardial biopsy; heart failure; immunoglobulin light chain; left ventricular hypertrophy; systemic amyloidosis; transthyretin.
Copyright: © 2022 The Author(s).
Conflict of interest statement
Ahmad Masri receives research grants from Pfizer, Ionis, Akcea, and Ultromics and fees from Eidos, Pfizer, Ionis, Akcea, Alnylam, Cytokinetics, BMS, Tenaya and Attralus. There are no other disclosures.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
