

Biodegradable magnesium implant enhances angiogenesis and alleviates medication-related osteonecrosis of the jaw in rats
- PMID: 35415073
- PMCID: PMC8965768
- DOI: 10.1016/j.jot.2022.03.004
Biodegradable magnesium implant enhances angiogenesis and alleviates medication-related osteonecrosis of the jaw in rats
Abstract
Background: Medication-related osteonecrosis of the jaw (MRONJ) is a serious complication associated with antiresorptive and antiangiogenic medications, of which impaired angiogenesis is a key pathological alteration. Since Magnesium (Mg)-based implants possess proangiogenic effects, we hypothesized that the biodegradable Mg implant could alleviate the development of MRONJ via enhancing angiogenesis.
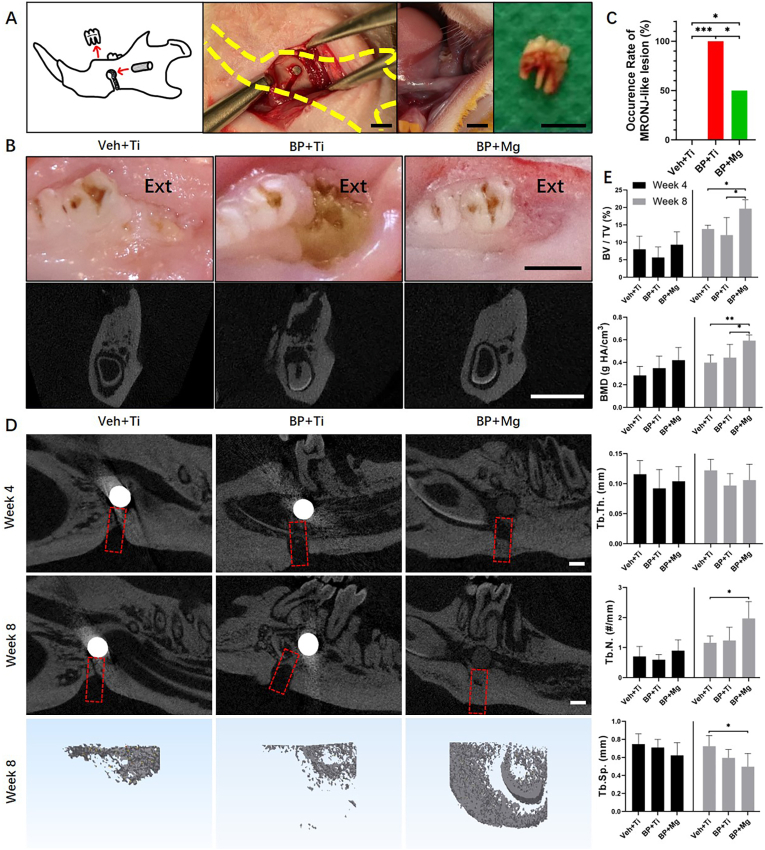
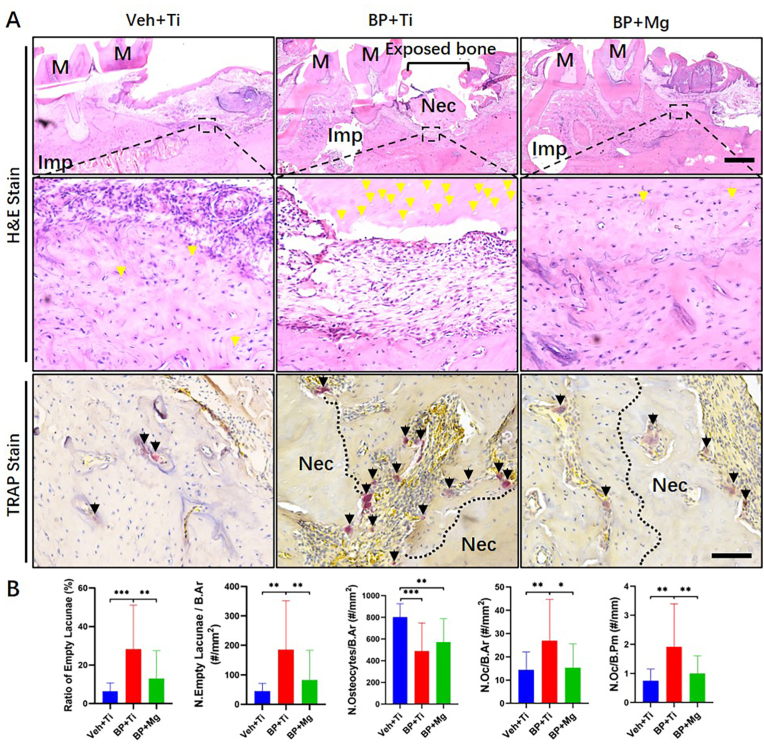
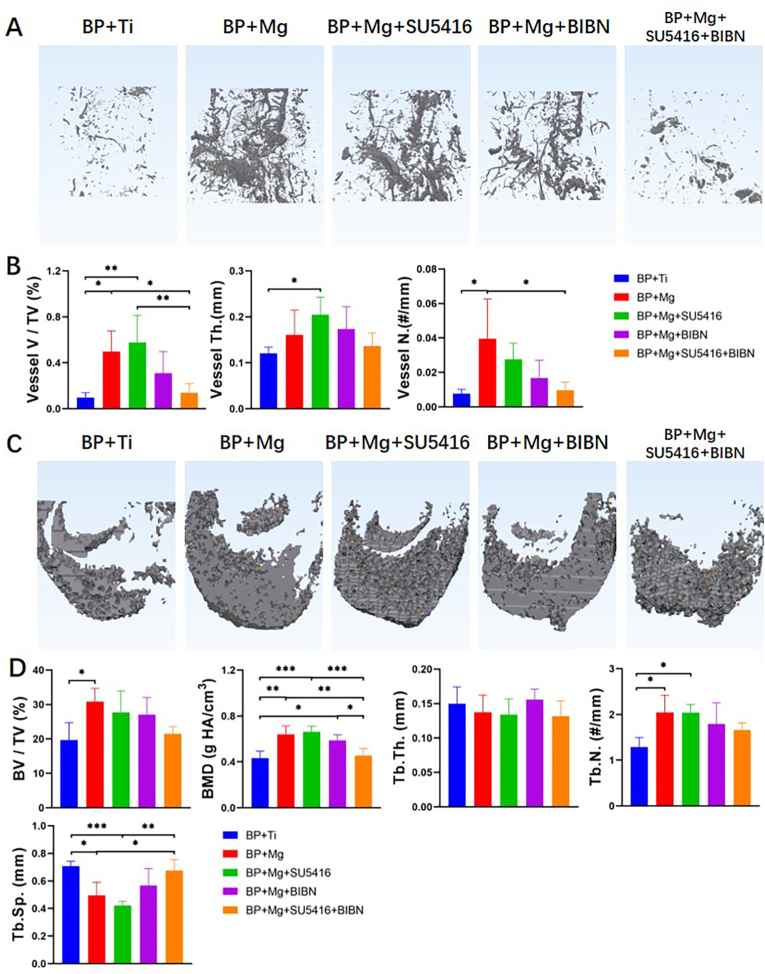
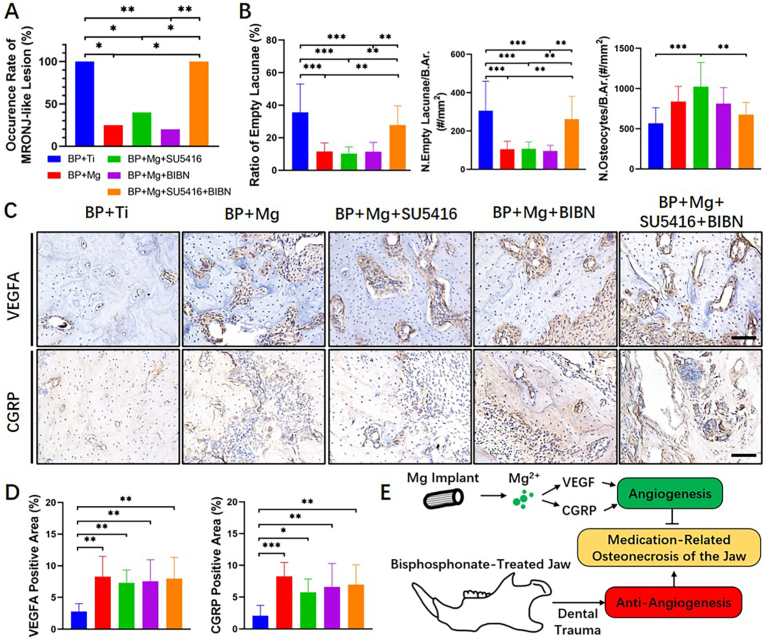
Methods: MRONJ model was established and divided into the Veh + Ti group (Vehicle-treated rat, with Titanium (Ti) implant), BP + Ti group (Bisphosphonate (BP)-treated rat, with Ti implant), BP + Mg group (BP-treated rat, with Mg implant), BP + Mg + SU5416 group (BP-treated rat, with Mg implant and vascular endothelial growth factor (VEGF) receptor-2 inhibitor), BP + Mg + BIBN group (BP-treated rat, with Mg implant and calcitonin gene-related peptide (CGRP) receptor antagonist), and BP + Mg + SU5416+BIBN group (BP-treated rat, with Mg implant and VEGF receptor-2 inhibitor and CGRP receptor antagonist). The occurrence of MRONJ, alveolar bone necrosis, new bone formation and vessel formation were assessed by histomorphometry, immunohistochemistry, and micro-CT analysis.
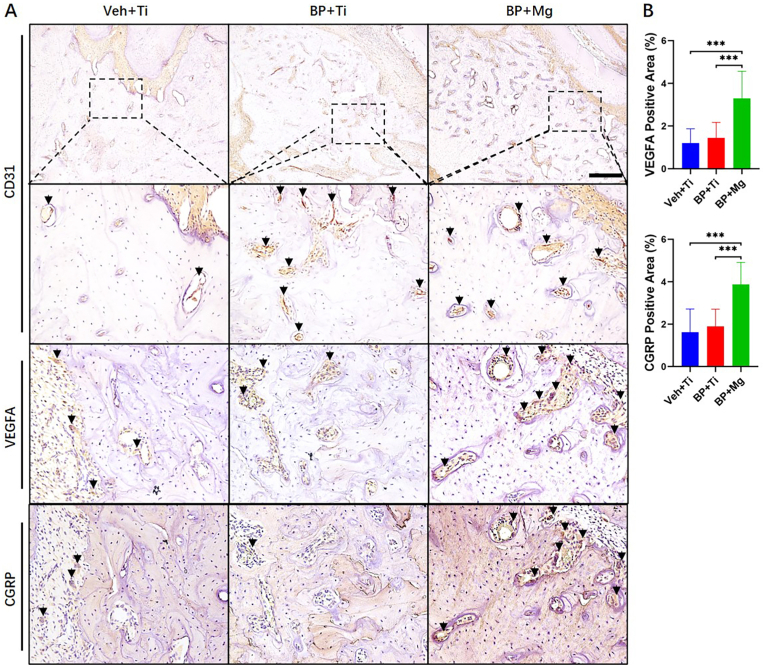
Results: Eight weeks after surgery, the BP + Mg group had significantly reduced occurrence of MRONJ-like lesion and histological osteonecrosis, increased bone microstructural parameters, and increased expressions of VEGFA and CGRP, than the BP + Ti group. By simultaneously blocking VEGF receptor-2 and CGRP receptor, the vessel volume and new bone formation in the BP + Mg group were significantly decreased, meanwhile the occurrence of MRONJ-like lesion and histological bone necrosis were significantly increased.
Conclusion: Biodegradable Mg implant could alleviate the development of MRONJ-like lesion, possibly via upregulating VEGF- and CGRP-mediated angiogenesis. Mg-based implants have the translational potential to be developed as a novel internal fixation device for patients with the risk of MRONJ.
The translational potential of this article: This work reports a biodegradable Mg implant which ameliorates the development of MRONJ-like lesions possibly due to its angiogenic property. Mg-based implants have the potential to be developed as a novel internal fixation device for patients at the risk of MRONJ.
Keywords: Angiogenesis; Biodegradable implants; Bisphosphonate; Magnesium; Medication-related osteonecrosis of the jaw.
© 2022 The Author(s).
Conflict of interest statement
The author(s) have no conflicts of interest relevant to this article.
Figures
References
-
- Ruggiero S.L., Dodson T.B., Fantasia J., Goodday R., Aghaloo T., Mehrotra B., et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J Oral Maxillofac Surg. 2014;72(10):1938–1956. - PubMed
-
- Otto S., Pautke C., Van den Wyngaert T., Niepel D., Schiodt M. Medication-related osteonecrosis of the jaw: prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treat Rev. 2018;69:177–187. - PubMed
-
- Coleman R., Woodward E., Brown J., Cameron D., Bell R., Dodwell D., et al. Safety of zoledronic acid and incidence of osteonecrosis of the jaw (ONJ) during adjuvant therapy in a randomised phase III trial (AZURE: BIG 01-04) for women with stage II/III breast cancer. Breast Cancer Res Treat. 2011;127(2):429–438. [eng] - PubMed
-
- Mauri D., Valachis A., Polyzos I.P., Polyzos N.P., Kamposioras K., Pesce L.L. Osteonecrosis of the jaw and use of bisphosphonates in adjuvant breast cancer treatment: a meta-analysis. Breast Cancer Res Treat. 2009;116(3):433–439. [eng] - PubMed
-
- Scagliotti G.V., Hirsh V., Siena S., Henry D.H., Woll P.J., Manegold C., et al. Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: subgroup analysis from a randomized phase 3 study. J Thorac Oncol : Off Publ Int Assoc Stud Lung Cancer. 2012;7(12):1823–1829. [eng] - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
