

Two-year follow-up after operative treatment of an osseous Bankart lesion with a flap-detached cartilage lesion of the glenoid: A case report
- PMID: 35416169
- PMCID: PMC9612653
- DOI: 10.5152/j.aott.2022.21271
Two-year follow-up after operative treatment of an osseous Bankart lesion with a flap-detached cartilage lesion of the glenoid: A case report
Abstract
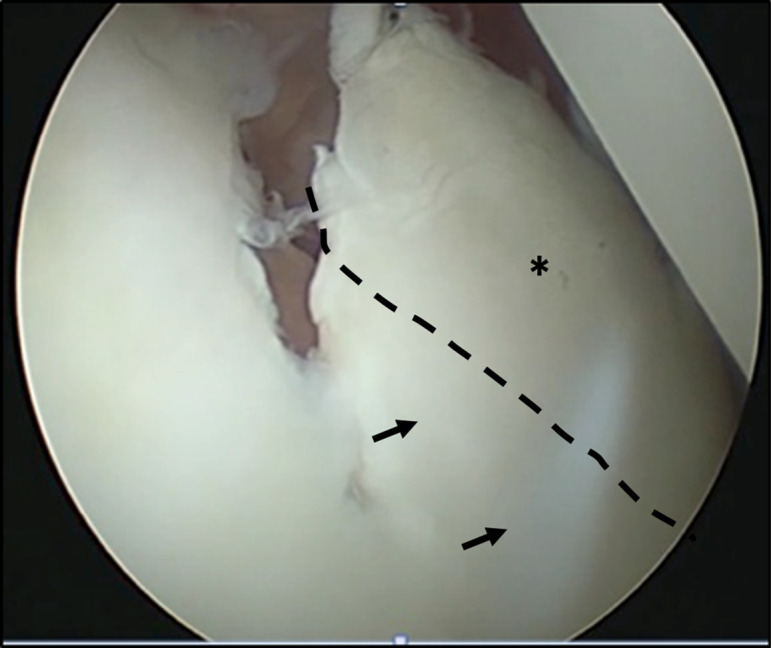
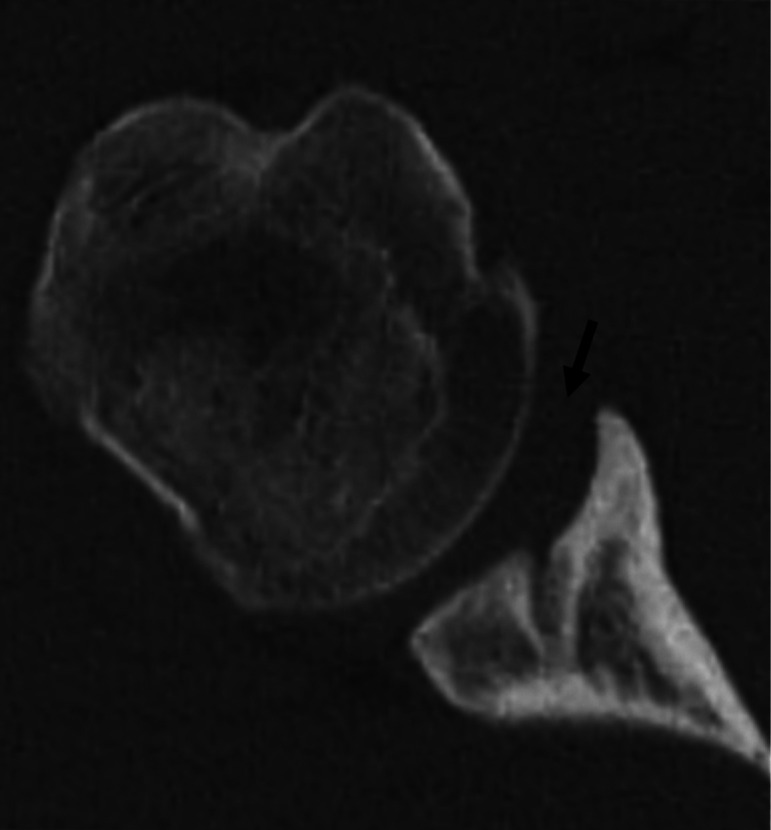
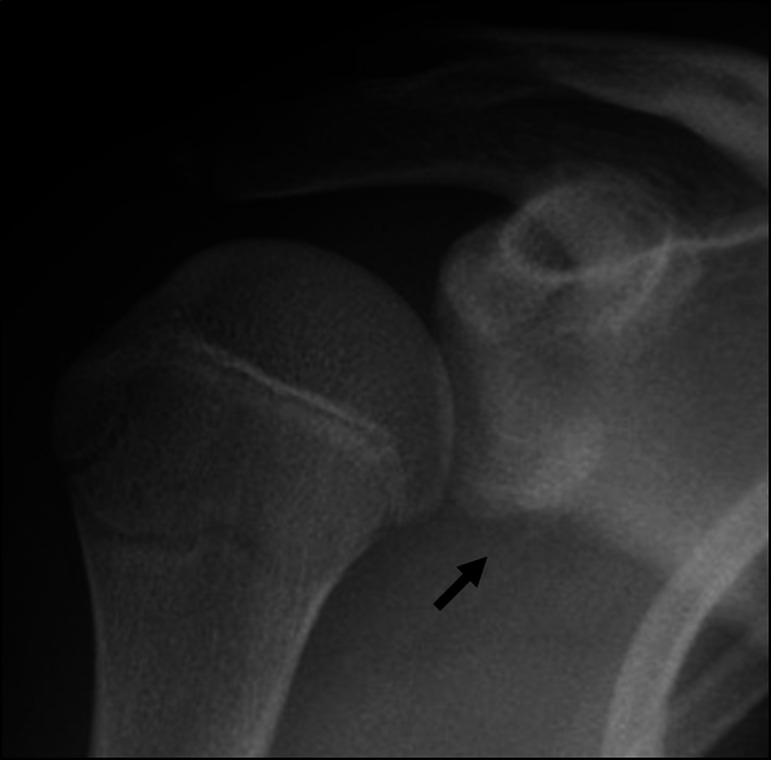
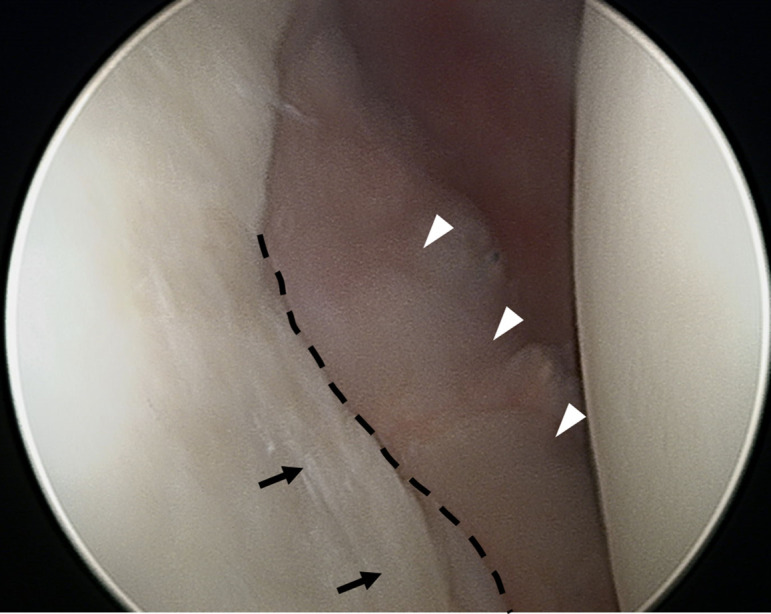
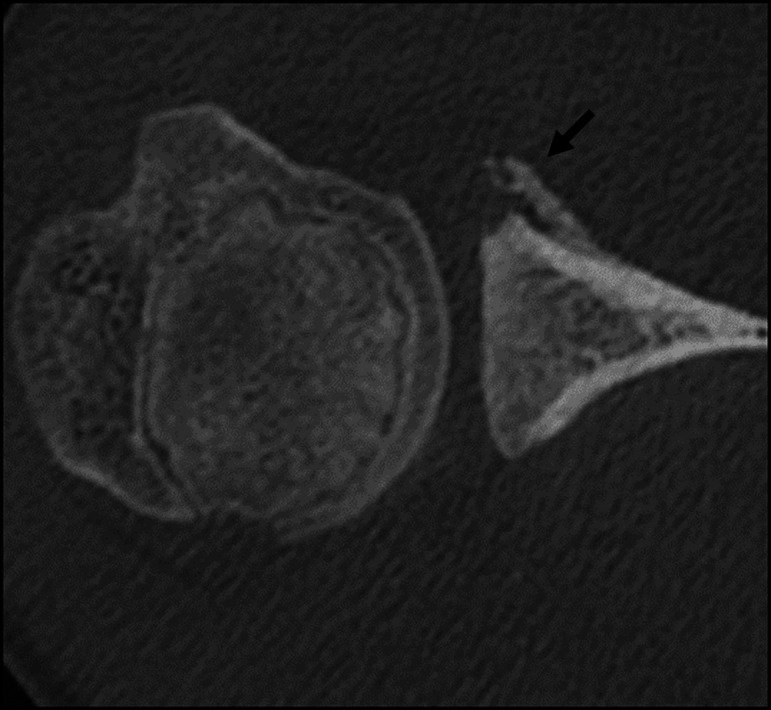
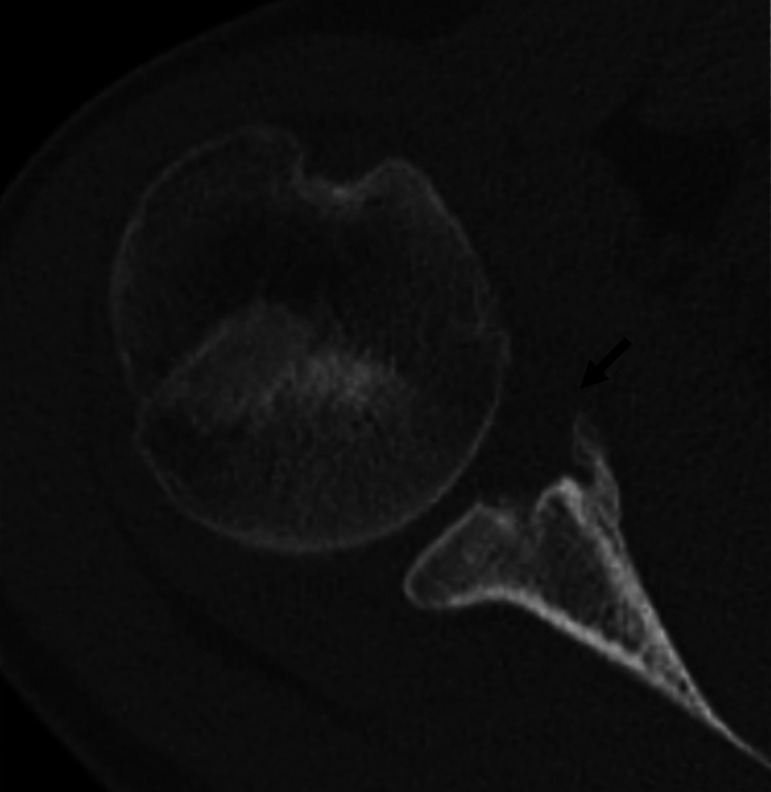
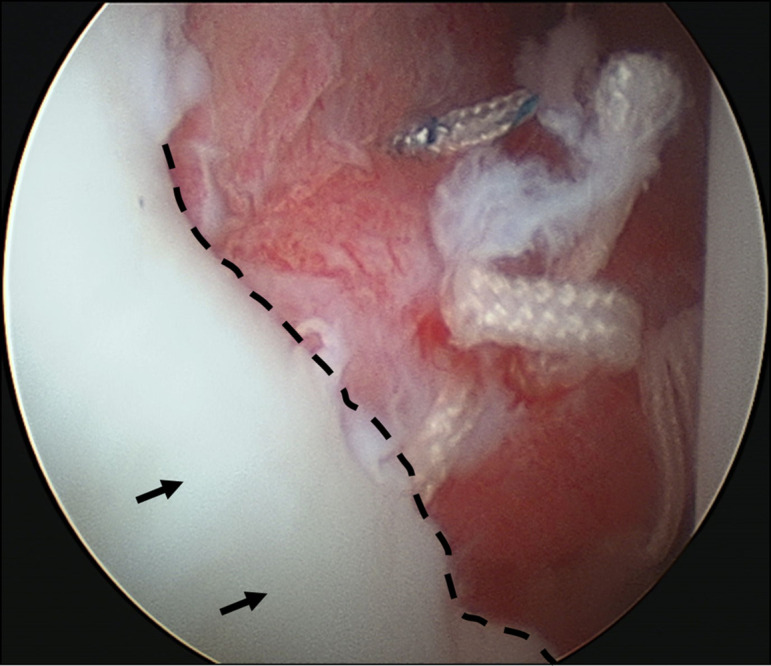
Glenoid articular cartilage lesion is a rare complication following traumatic anterior dislocation of the shoulder. We report the case of a 14-year-old male rugby player with traumatic anterior shoulder instability, an extensively flapped lesion on the glenoid articular cartilage, and an osseous Bankart lesion. Arthroscopic findings revealed that the glenoid cartilage was flap-detached, extending from the anteroinferior to the center. Repair of the osseous Bankart lesion using suture anchors and resection of the unstable peripheral part of the cartilage was performed arthroscopically. The main region of the injured articular surface was left untouched. During postoperative follow-up, absorption of the glenoid articular surface near the suture anchor holes was identified. Arthroscopic examination three months post-surgery showed that the flap detached lesion of the residual cartilage was stable and appeared adapted on the glenoid surface. The resected area was covered by fibrous tissue. A follow-up computed tomography scan revealed that the osseous lesion was united. The patient returned to his previous sports capacity eight months following the operation. At the 2-year-follow-up, magnetic resonance imaging revealed that the glenoid surface was remodeled to a flattened round shape with no signs of osteoarthritis, exhibiting proper conformity of the joint surfaces to the humeral head. Arthroscopic Bankart repair using suture anchors may cause bone resorption at the glenoid surface, leading to remodeling of the glenoid surface from the damaged glenoid cartilage lesion in young patients.
Figures

References
-
- Tasaki A, Morita W, Yamakawa A.et al. Combined arthroscopic Bankart repair and coracoid process transfer to anterior glenoid for shoulder dislocation in rugby players: evaluation based on ability to perform sport-specific movements effectively. Arthroscopy. 2015;31(9):1693 1701. 10.1016/j.arthro.2015.03.013) - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
