

Superior mesenteric vein reconstruction during pancreatoduodenectomy using a dilated right ovarian vein in a patient at future risk for pelvic congestion syndrome: a case report
- PMID: 35416521
- PMCID: PMC9008091
- DOI: 10.1186/s40792-022-01421-w
Superior mesenteric vein reconstruction during pancreatoduodenectomy using a dilated right ovarian vein in a patient at future risk for pelvic congestion syndrome: a case report
Abstract
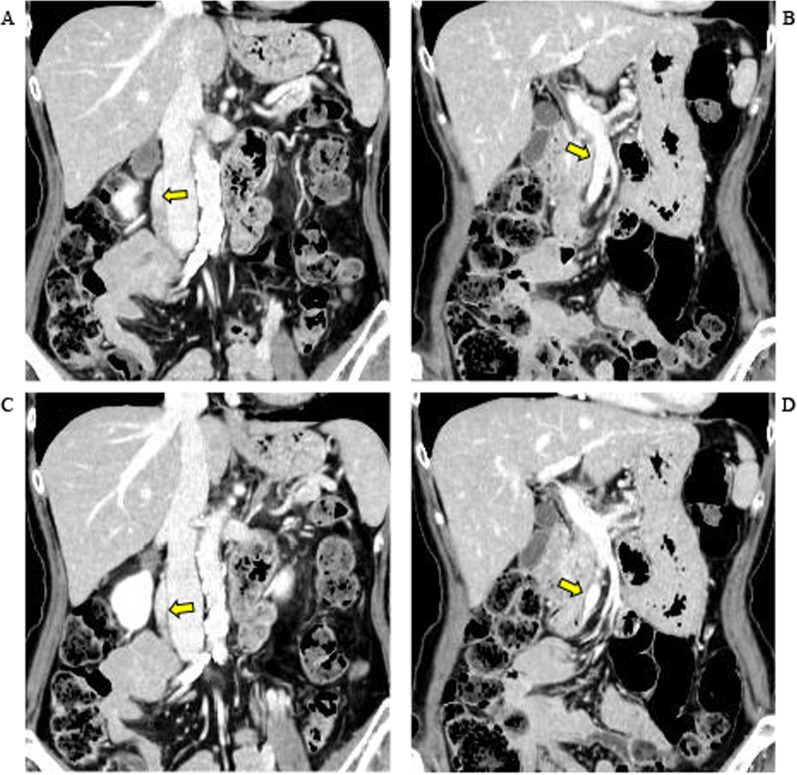
Background: Pancreatoduodenectomy including resection of the superior mesenteric vein (SMV) is increasingly performed for right-sided pancreatic ductal adenocarcinoma invading the wall of that vessel. Various venous grafts may be chosen for reconstruction. We present a woman with pancreatic cancer who underwent such a pancreatoduodenectomy with venous reconstruction using a dilated right ovarian vein.
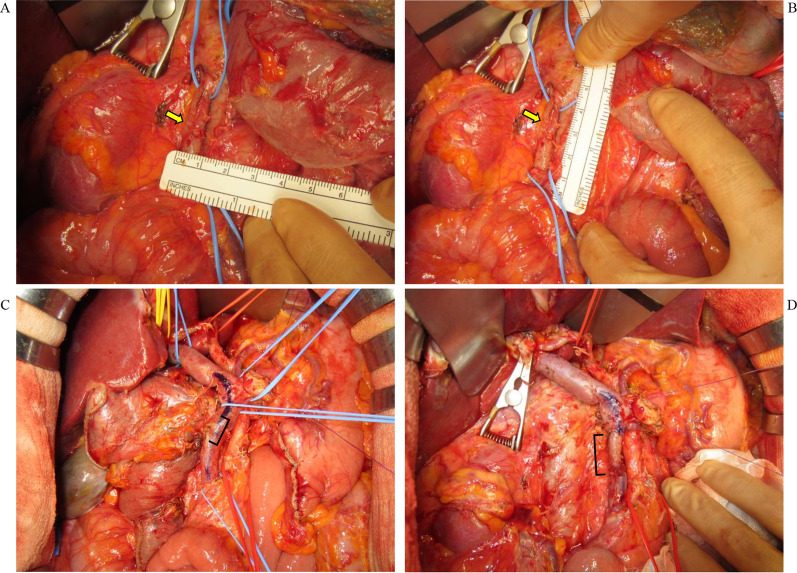
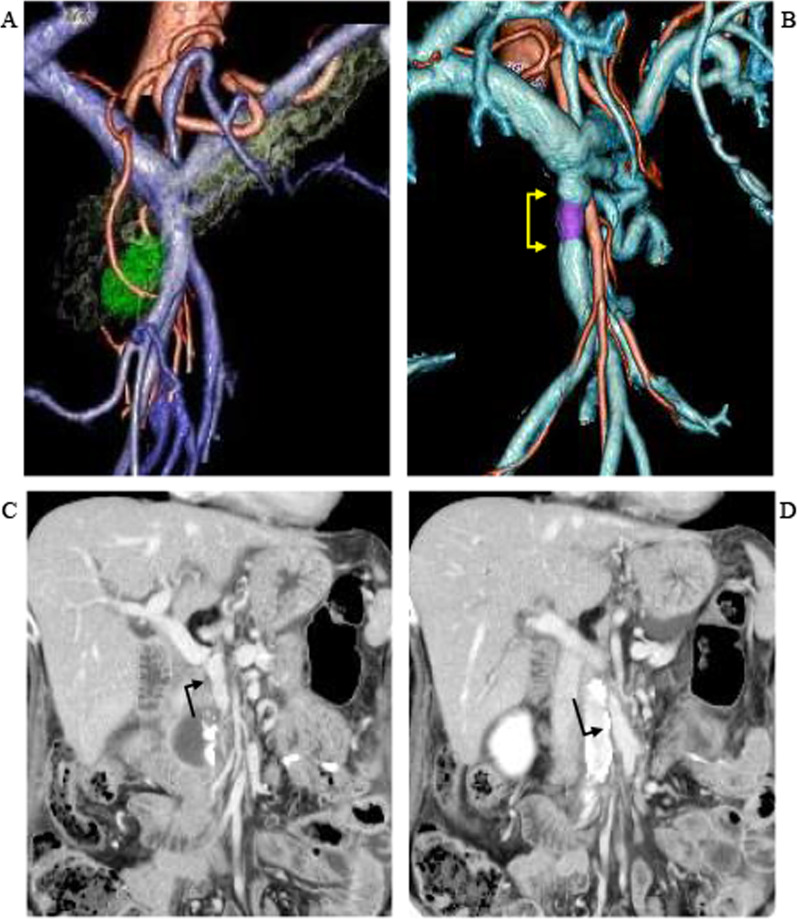
Case presentation: A 71-year-old woman with cancer involving the pancreatic head, uncinate process, and SMV underwent pancreatoduodenectomy with SMV resection. Reconstruction used a portion of the right ovarian vein that was markedly dilated and had placed her at risk for pelvic congestion syndrome (PCS). Graft patency was confirmed 8 months after surgery. She now finished receiving adjuvant chemotherapy and has no symptoms of PCS.
Conclusion: If an ovarian vein has sufficient diameter, it can be used to reconstruct the resected segment of the SMV during pancreatoduodenectomy in suitable patients.
Keywords: Pancreatoduodenectomy; Pelvic congestion syndrome; Superior mesenteric vein resection and reconstruction.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources
