

Long-term Quality of Life in Patients With Breast Cancer After Breast Conservation vs Mastectomy and Reconstruction
- PMID: 35416926
- PMCID: PMC9008558
- DOI: 10.1001/jamasurg.2022.0631
Long-term Quality of Life in Patients With Breast Cancer After Breast Conservation vs Mastectomy and Reconstruction
Abstract
Importance: Treatment options for early breast cancer include breast-conserving surgery with radiation therapy (RT) or mastectomy and breast reconstruction without RT. Despite marked differences in these treatment strategies, little is known with regard to their association with long-term quality of life (QOL).
Objective: To evaluate the association of treatment with breast-conserving surgery with RT vs mastectomy and reconstruction without RT with long-term QOL.
Design, setting, and participants: This comparative effectiveness research study used data from the Texas Cancer Registry for women diagnosed with stage 0-II breast cancer and treated with breast-conserving surgery or mastectomy and reconstruction between 2006 and 2008. The study sample was mailed a survey between March 2017 and April 2018. Data were analyzed from August 1, 2018 to October 15, 2021.
Exposures: Breast-conserving surgery with RT or mastectomy and reconstruction without RT.
Main outcomes and measures: The primary outcome was satisfaction with breasts, measured with the BREAST-Q patient-reported outcome measure. Secondary outcomes included BREAST-Q physical well-being, psychosocial well-being, and sexual well-being; health utility, measured using the EuroQol Health-Related Quality of Life 5-Dimension, 3-Level questionnaire; and local therapy decisional regret. Multivariable linear regression models with weights for treatment, age, and race and ethnicity tested associations of the exposure with outcomes.
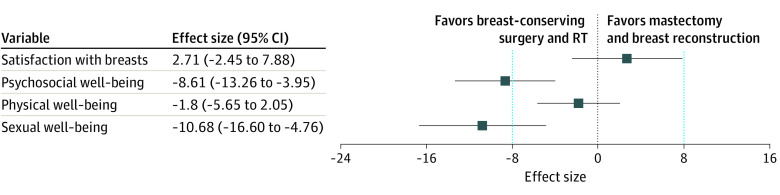
Results: Of 647 patients who responded to the survey (40.0%; 356 had undergone breast-conserving surgery, and 291 had undergone mastectomy and reconstruction), 551 (85.2%) confirmed treatment with breast-conserving surgery with RT (n = 315) or mastectomy and reconstruction without RT (n = 236). Among the 647 respondents, the median age was 53 years (range, 23-85 years) and the median time from diagnosis to survey was 10.3 years (range, 8.4-12.5 years). Multivariable analysis showed no significant difference between breast-conserving surgery with RT (referent) and mastectomy and reconstruction without RT in satisfaction with breasts (effect size, 2.71; 95% CI, -2.45 to 7.88; P = .30) or physical well-being (effect size, -1.80; 95% CI, -5.65 to 2.05; P = .36). In contrast, psychosocial well-being (effect size, -8.61; 95% CI, -13.26 to -3.95; P < .001) and sexual well-being (effect size, -10.68; 95% CI, -16.60 to -4.76; P < .001) were significantly worse with mastectomy and reconstruction without RT. Health utility (effect size, -0.003; 95% CI, -0.03 to 0.03; P = .83) and decisional regret (effect size, 1.32; 95% CI, -3.77 to 6.40; P = .61) did not differ by treatment group.
Conclusions and relevance: The findings support equivalence of breast-conserving surgery with RT and mastectomy and reconstruction without RT with regard to breast satisfaction and physical well-being. However, breast-conserving surgery with RT was associated with clinically meaningful improvements in psychosocial and sexual well-being. These findings may help inform preference-sensitive decision-making for women with early-stage breast cancer.
Conflict of interest statement
Figures
Comment in
-
Association of Breast-Conserving Therapy With Measures of Long-term Quality of Life Compared With Mastectomy and Reconstruction.JAMA Surg. 2022 Jun 1;157(6):e220637. doi: 10.1001/jamasurg.2022.0637. Epub 2022 Jun 8. JAMA Surg. 2022. PMID: 35416916 No abstract available.
References
-
- Clarke M, Collins R, Darby S, et al. ; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) . Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087-2106. doi:10.1016/S0140-6736(05)67887-7 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
