

Practical outpatient management of worsening chronic heart failure
- PMID: 35417093
- PMCID: PMC9325366
- DOI: 10.1002/ejhf.2503
Practical outpatient management of worsening chronic heart failure
Abstract
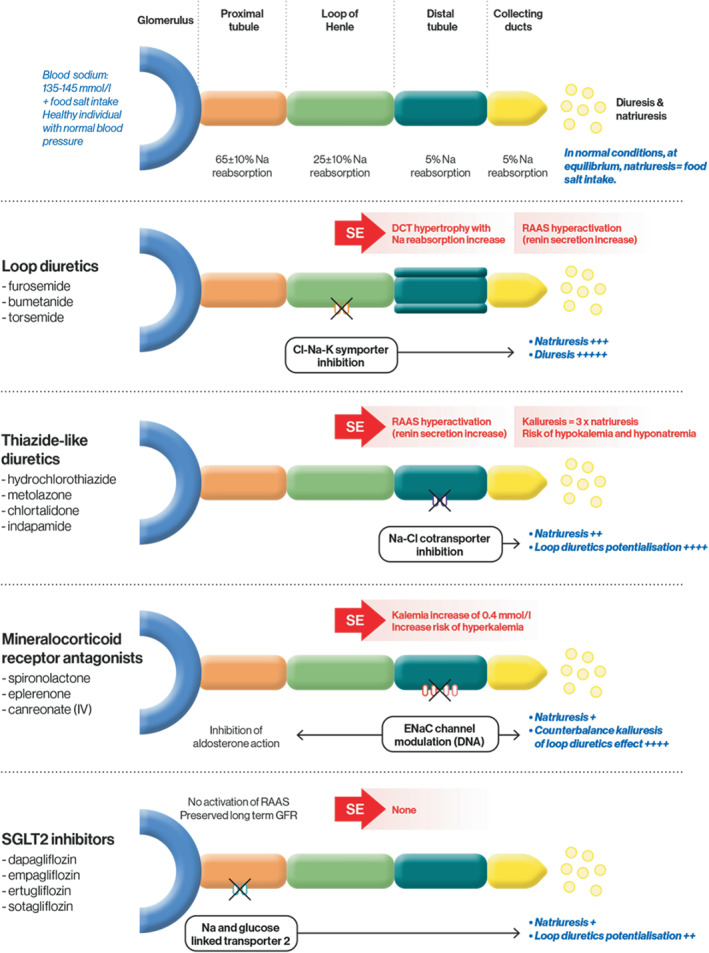
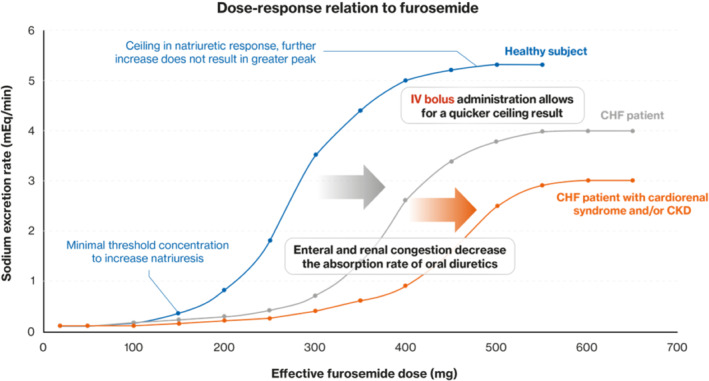
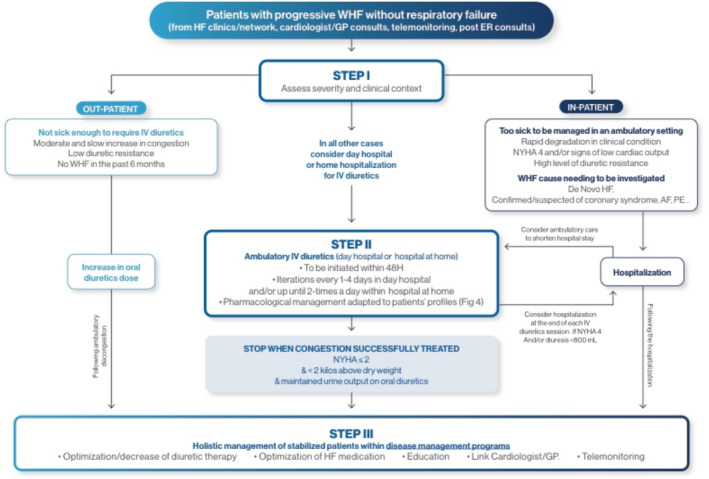
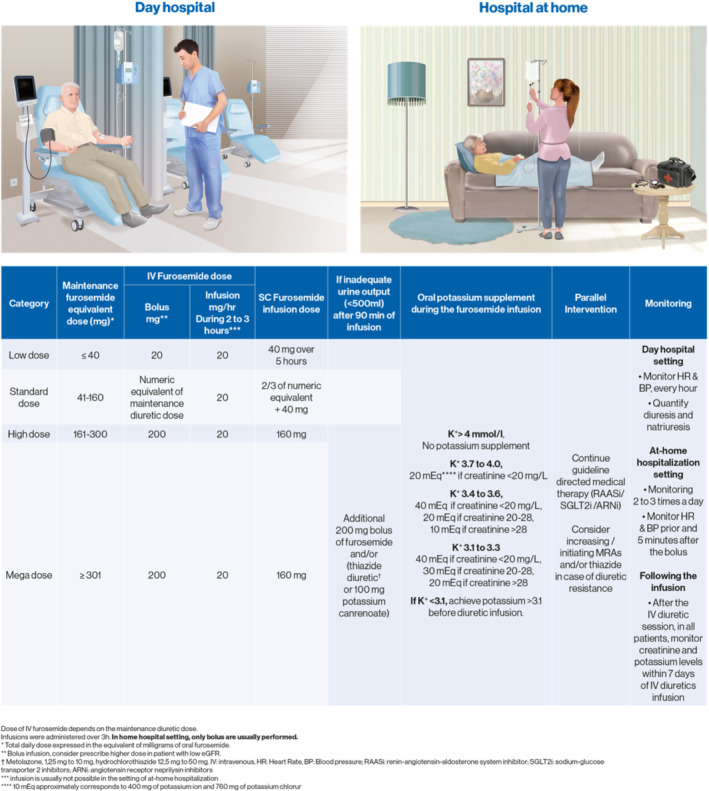
Management of worsening heart failure (WHF) has traditionally been hospital-based, but with the rising burden of heart failure (HF), the pressure on healthcare systems exerted by this disease necessitates a different strategy than long (and costly) hospital stays. A strategy for outpatient intravenous (IV) diuretic treatment of WHF has been developed in certain American centres in the past 10 years, whereas European centres have been mostly favouring 'classic' in-hospital management of WHF. Embracing novel, outpatient approaches for treating WHF could substantially reduce the burden on healthcare systems while improving patient's satisfaction and quality of life. The present article is intended to provide essential knowledge and practical guidelines aimed at helping clinicians implement these new ambulatory approaches using day hospital and/or at-home hospitalization. The topics addressed by our group of HF experts include the pathophysiological background of diuretic therapy, the most suitable profile of WHF that may be managed in an ambulatory setting, the pharmacological protocols that can be used, as well as a detailed description of healthcare structures that can be proposed to deliver these ambulatory care interventions. The practical aspects of day hospital and hospital-at-home IV diuretic administration are specifically emphasized. The algorithm provided along with the practical IV diuretic protocols should assist HF clinicians in implementing this new approach in their local clinical setting.
Keywords: Ambulatory management; Cardiac congestion; Cardiovascular diseases; Diuretics; Heart failure.
© 2022 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
References
-
- Zakeri R, Cowie MR. Heart failure with preserved ejection fraction: controversies, challenges and future directions. Heart. 2018;104:377–84. - PubMed
-
- van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail. 2016;18:242–52. - PubMed
-
- Braunwald E. Heart failure. JACC Heart Fail. 2013;1:1–20. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
