

Predicting the earliest deviation in weight gain in the course towards manifest overweight in offspring exposed to obesity in pregnancy: a longitudinal cohort study
- PMID: 35418073
- PMCID: PMC9008920
- DOI: 10.1186/s12916-022-02318-z
Predicting the earliest deviation in weight gain in the course towards manifest overweight in offspring exposed to obesity in pregnancy: a longitudinal cohort study
Abstract
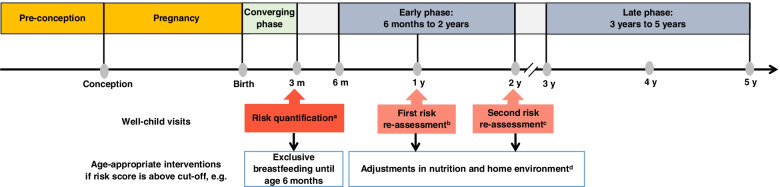
Background: Obesity in pregnancy and related early-life factors place the offspring at the highest risk of being overweight. Despite convincing evidence on these associations, there is an unmet public health need to identify "high-risk" offspring by predicting very early deviations in weight gain patterns as a subclinical stage towards overweight. However, data and methods for individual risk prediction are lacking. We aimed to identify those infants exposed to obesity in pregnancy at ages 3 months, 1 year, and 2 years who likely will follow a higher-than-normal body mass index (BMI) growth trajectory towards manifest overweight by developing an early-risk quantification system.
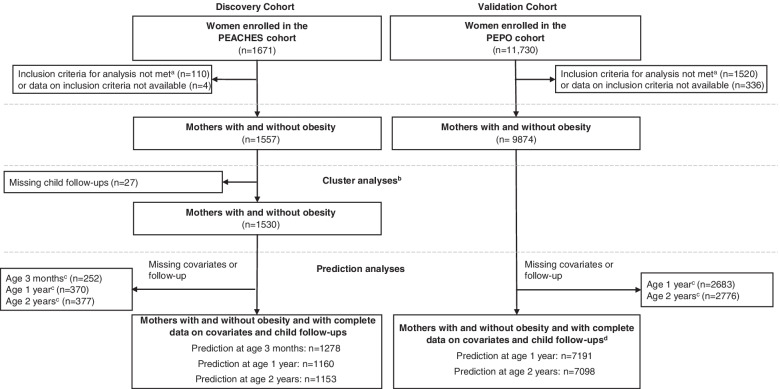
Methods: This study uses data from the prospective mother-child cohort study Programming of Enhanced Adiposity Risk in CHildhood-Early Screening (PEACHES) comprising 1671 mothers with pre-conception obesity and without (controls) and their offspring. Exposures were pre- and postnatal risks documented in patient-held maternal and child health records. The main outcome was a "higher-than-normal BMI growth pattern" preceding overweight, defined as BMI z-score >1 SD (i.e., World Health Organization [WHO] cut-off "at risk of overweight") at least twice during consecutive offspring growth periods between age 6 months and 5 years. The independent cohort PErinatal Prevention of Obesity (PEPO) comprising 11,730 mother-child pairs recruited close to school entry (around age 6 years) was available for data validation. Cluster analysis and sequential prediction modelling were performed.
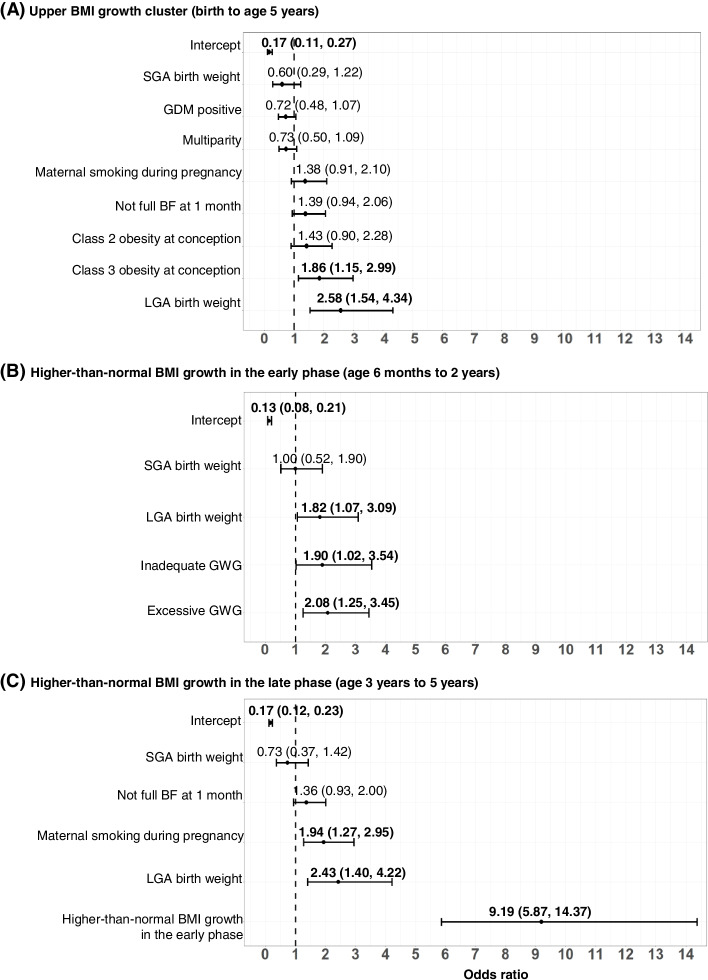
Results: Data of 1557 PEACHES mother-child pairs and the validation cohort were analyzed comprising more than 50,000 offspring BMI measurements. More than 1-in-5 offspring exposed to obesity in pregnancy belonged to an upper BMI z-score cluster as a distinct pattern of BMI development (above the cut-off of 1 SD) from the first months of life onwards resulting in preschool overweight/obesity (age 5 years: odds ratio [OR] 16.13; 95% confidence interval [CI] 9.98-26.05). Contributing early-life factors including excessive weight gain (OR 2.08; 95% CI 1.25-3.45) and smoking (OR 1.94; 95% CI 1.27-2.95) in pregnancy were instrumental in predicting a "higher-than-normal BMI growth pattern" at age 3 months and re-evaluating the risk at ages 1 year and 2 years (area under the receiver operating characteristic [AUROC] 0.69-0.79, sensitivity 70.7-76.0%, specificity 64.7-78.1%). External validation of prediction models demonstrated adequate predictive performances.
Conclusions: We devised a novel sequential strategy of individual prediction and re-evaluation of a higher-than-normal weight gain in "high-risk" infants well before developing overweight to guide decision-making. The strategy holds promise to elaborate interventions in an early preventive manner for integration in systems of well-child care.
Keywords: BMI growth; Early prevention; Early weight gain; Infancy; Maternal pre-conception obesity; Repeated risk assessment; Sequential prediction; Subclinical stage.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
