

Interface astrogliosis in contact sport head impacts and military blast exposure
- PMID: 35418116
- PMCID: PMC9009003
- DOI: 10.1186/s40478-022-01358-z
Interface astrogliosis in contact sport head impacts and military blast exposure
Abstract
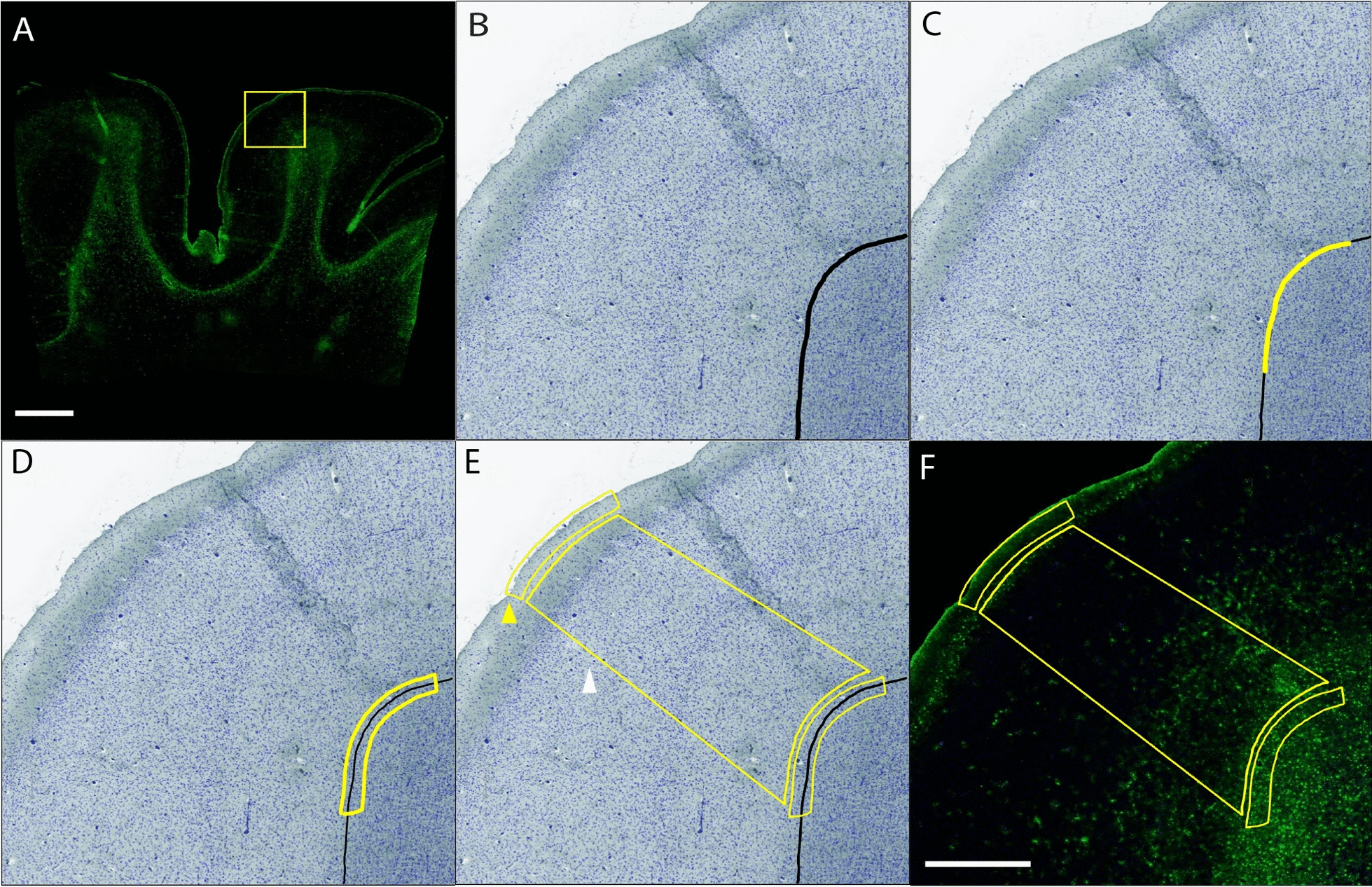
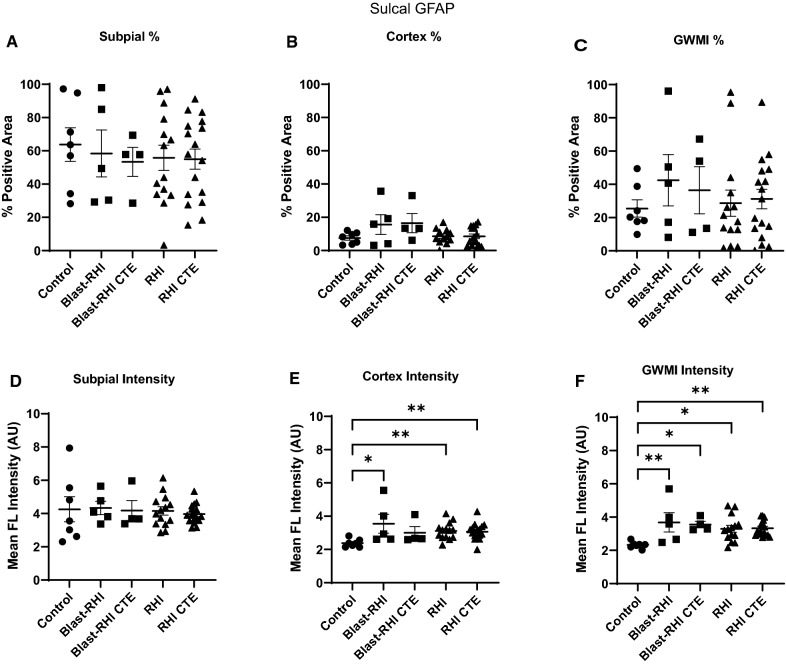
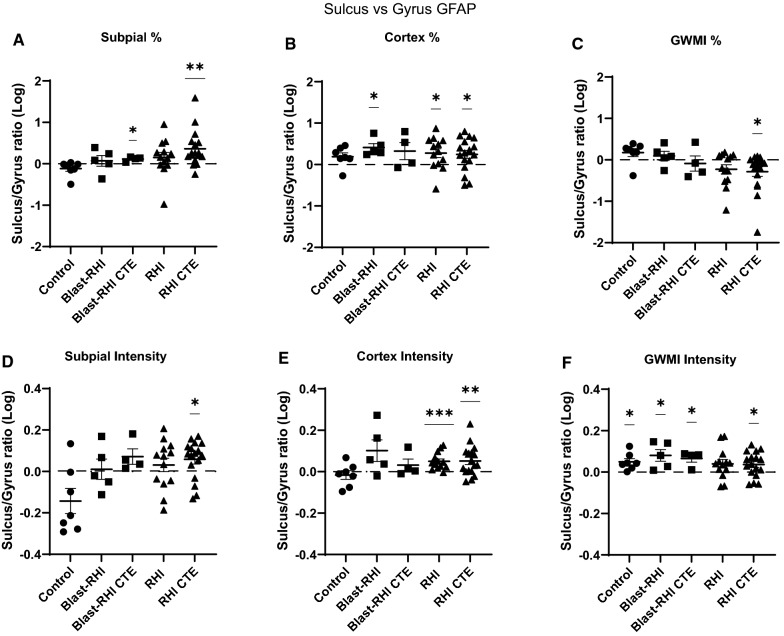
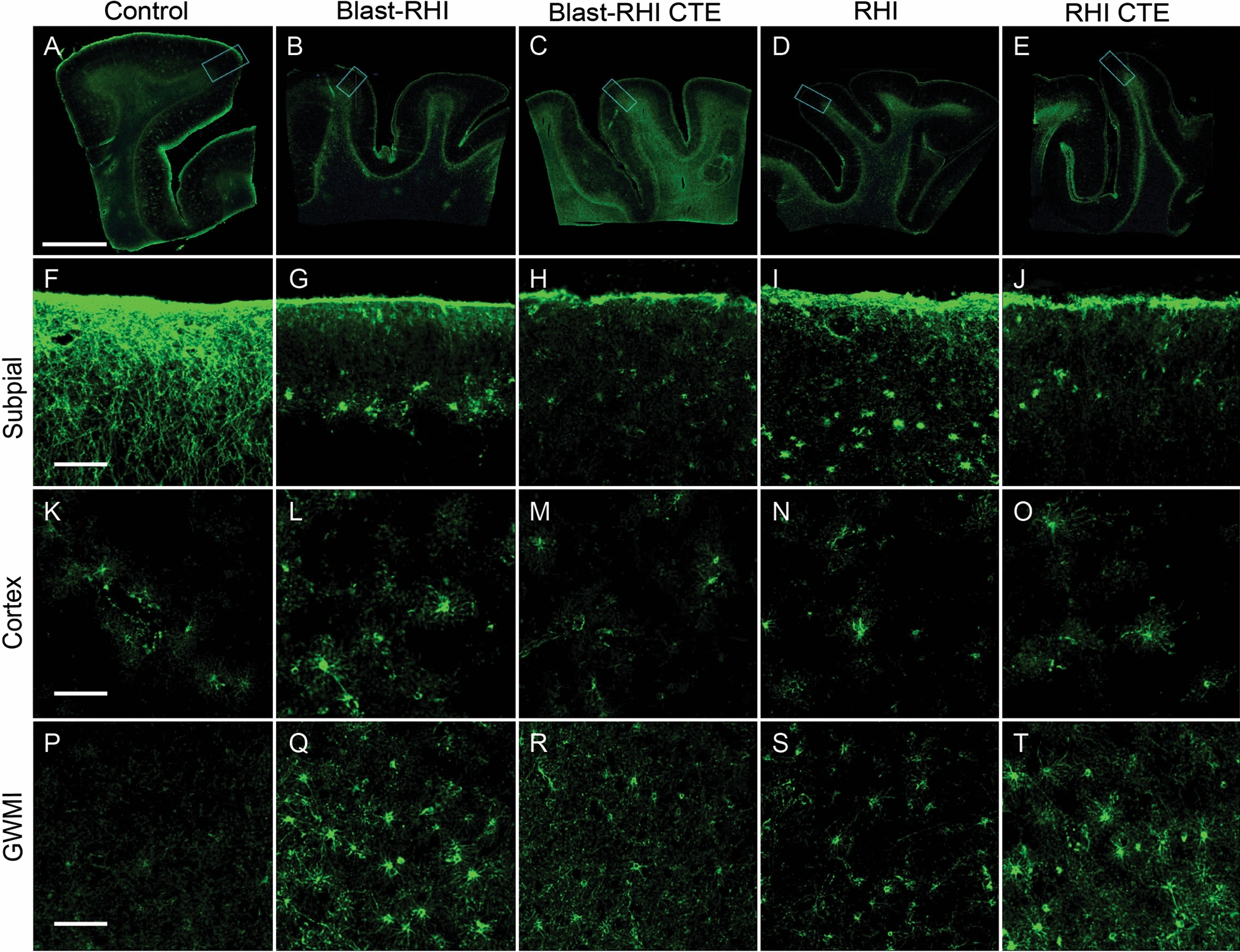
Exposure to military blast and repetitive head impacts (RHI) in contact sports is associated with increased risk of long-term neurobehavioral sequelae and cognitive deficits, and the neurodegenerative disease chronic traumatic encephalopathy (CTE). At present, the exact pathogenic mechanisms of RHI and CTE are unknown, and no targeted therapies are available. Astrocytes have recently emerged as key mediators of the multicellular response to head trauma. Here, we investigated interface astrogliosis in blast and impact neurotrauma, specifically in the context of RHI and early stage CTE. We compared postmortem brain tissue from former military veterans with a history of blast exposure with and without a neuropathological diagnosis of CTE, former American football players with a history of RHI with and without a neuropathological diagnosis of CTE, and control donors without a history of blast, RHI exposure or CTE diagnosis. Using quantitative immunofluorescence, we found that astrogliosis was higher at the grey-white matter interface in the dorsolateral frontal cortex, with mixed effects at the subpial surface and underlying cortex, in both blast and RHI donors with and without CTE, compared to controls. These results indicate that certain astrocytic alterations are associated with both impact and blast neurotrauma, and that different astroglial responses take place in distinct brain regions.
Keywords: Astrogliosis; Blast injury; Chronic traumatic encephalopathy; Mild traumatic brain injury; Repetitive head impacts.
© 2022. The Author(s).
Conflict of interest statement
The authors have no duality or conflicts of interest to declare.
Figures


References
-
- Bieniek KF, Cairns NJ, Crary JF, Dickson DW, Folkerth RD, Keene CD, et al. The second NINDS/nibib consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. J Neuropathol Exp Neurol. 2021;80:210–219. doi: 10.1007/s00401-015-1515-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
