

Bedside intra-aortic balloon pump insertion in cardiac intensive care unit: A single-center experience
- PMID: 35419933
- PMCID: PMC9544237
- DOI: 10.1002/ccd.30197
Bedside intra-aortic balloon pump insertion in cardiac intensive care unit: A single-center experience
Abstract
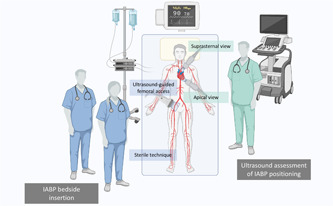
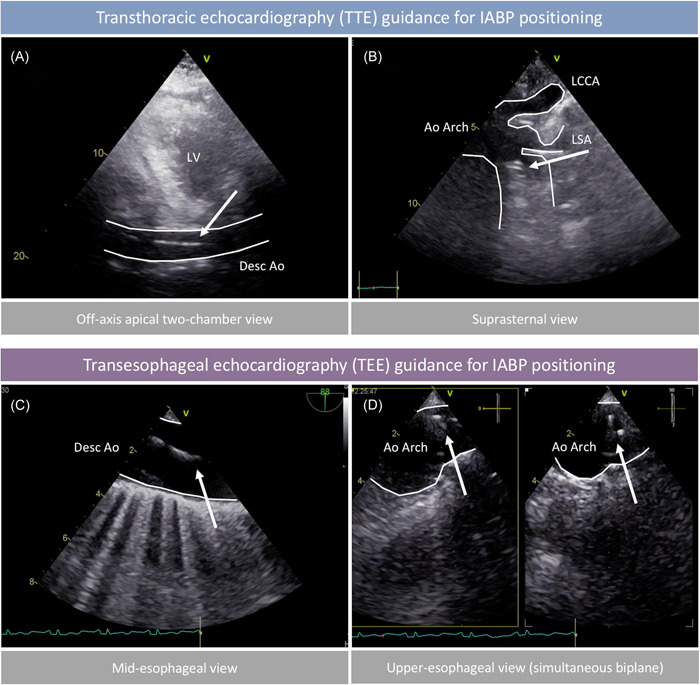
Background: In contemporary Cardiac Intensive Care Unit (CICU), bedside intra-aortic balloon pump (IABP) insertion under echocardiographic guidance may be an attractive option for selected patients with cardiogenic shock (CS). Currently available data on this approach are limited.
Aim: This study aimed to assess the feasibility and safety of bedside IABP insertion, as compared to fluoroscopic-guided insertion in the Catheterization Laboratory (CathLab), and to describe the clinical features of patients receiving bedside IABP insertion using a standardized technique in real-world CICU practice.
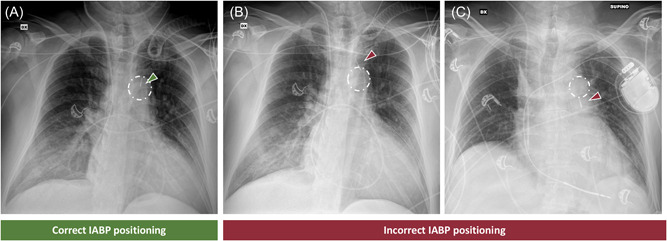
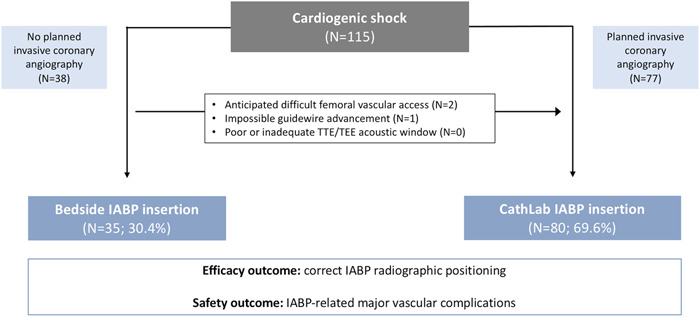
Methods: We prospectively evaluated all patients admitted the CICU who received transfemoral IABP between June 2020 and October 2021. The overall study cohort was divided according to implant strategy in bedside and CathLab groups. The primary outcome was correct radiographic IABP positioning at the first bedside chest X-ray obtained after insertion. Secondary outcomes included IABP-related complications.
Results: Among 115 patients, bedside IABP insertion was performed in 35 (30.4%) cases, mainly presenting with CS-related to acute decompensated heart failure (ADHF) (68.6 vs 33.8%; p < 0.001), with lower LVEF, higher proportion of right ventricular involvement and higher need of inotropes/vasopressors, compared to those receiving CathLab insertion. Bedside IABP insertion resulted feasible and safe, with similar rates of correct IABP positioning (82.9 vs. 82.5%; p = 0.963) and IABP-related major vascular complications (5.7 vs. 5.0%; p = 0.874), as compared to CathLab positioning.
Conclusion: This study suggests the feasibility and safety of bedside IABP insertion, which could be of relevant interest in patients with ADHF-related CS who may not need coronary angiography or other urgent CathLab procedures.
Keywords: IABP; bedside; cardiogenic shock; echocardiography; intra-aortic balloon pump.
© 2022 The Authors. Catheterization and Cardiovascular Interventions published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
