

Biosimilar Insulin Aspart Premix SAR341402 Mix 70/30 Versus Originator Insulin Aspart Mix 70/30 (NovoMix 30) in People with Diabetes: A 26-Week, Randomized, Open-Label Trial (GEMELLI M)
- PMID: 35420397
- PMCID: PMC9008602
- DOI: 10.1007/s13300-022-01255-7
Biosimilar Insulin Aspart Premix SAR341402 Mix 70/30 Versus Originator Insulin Aspart Mix 70/30 (NovoMix 30) in People with Diabetes: A 26-Week, Randomized, Open-Label Trial (GEMELLI M)
Abstract
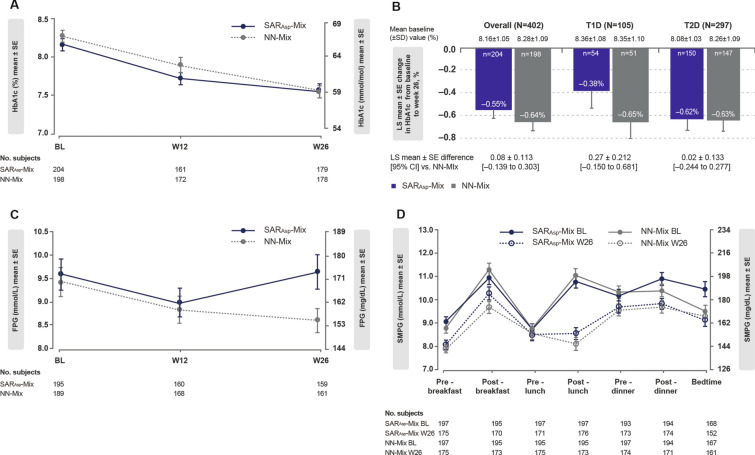
Introduction: This study compared the efficacy, safety, and immunogenicity of biosimilar insulin aspart premix SAR341402 Mix 70/30 (SARAsp-Mix) with European-approved insulin aspart mix 70/30 - NovoMix® 30 (NN-Mix) in people with type 1 (T1D) or type 2 diabetes (T2D).
Methods: This 26-week, open-label, phase 3 trial enrolled 402 people with T1D (n = 105) or T2D (n = 297) previously treated with premix insulin, who were randomized (1:1) to SARAsp-Mix (n = 204) or NN-Mix (n = 198).
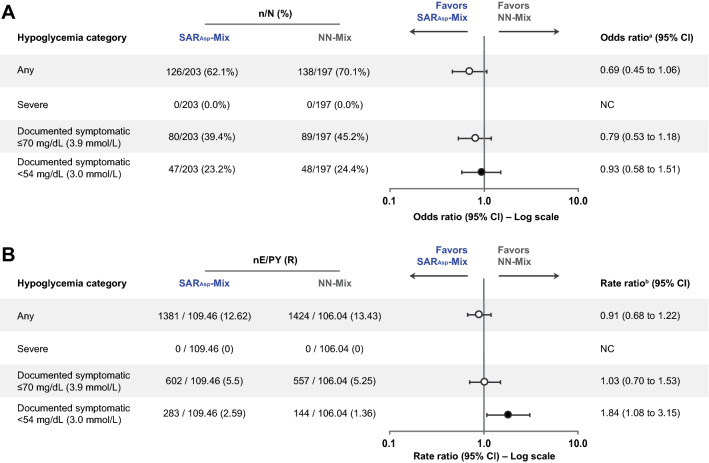
Results: After 26 weeks, the least squares (LS) mean [median] change in HbA1c from baseline was similar in both treatment groups (SARAsp-Mix - 0.55% [- 0.60%]; NN-Mix - 0.64% [- 0.60%]). The LS mean difference for SARAsp-Mix versus NN-Mix was 0.08%, with the upper bound of the two-sided 95% confidence interval (- 0.139 to 0.303) slightly above the prespecified noninferiority margin of 0.3%. Noninferiority of SARAsp-Mix over NN-Mix was not demonstrated in the primary intent-to-treat analysis, primarily because of one extreme outlying value impacted by the COVID-19 pandemic in the SARAsp-Mix group. Noninferiority was achieved in all secondary analyses, including prespecified per-protocol supportive and COVID-19 sensitivity analyses, as well as post hoc sensitivity analyses. Other efficacy endpoints, insulin dosages, anti-insulin aspart antibody response, hypoglycemia, and adverse events were similar between groups.
Conclusions: The totality of evidence indicates that SARAsp-Mix provides effective glycemic control with a similar safety and immunogenicity profile to NN-Mix in people with diabetes treated for 26 weeks.
Trial registration: EudraCT number 2017-000092-84.
Keywords: Biosimilar; GEMELLI M; Insulin aspart mix; Premix; SAR341402.
© 2022. The Author(s).
Figures

References
-
- Novo Nordisk: NovoLog Mix 70/30 insulin aspart protamine and insulin aspart injectable suspension 100 units/mL, NovoNordisk. Prescribing Information, revised: 4/2021. https://www.novo-pi.com/novologmix7030.pdf Accessed 3 Dec 2021.
-
- European Medicines Agency: NovoMix 30 (30% insulin aspart and 70% insulin aspart protamine). Summary of product characteristics, updated 12 November 2020. https://www.ema.europa.eu/en/documents/product-information/novomix-epar-... Accessed 3 Dec 2021.
-
- American Diabetes Association, Draznin B, Aroda VR, et al. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45:S125–S43. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
