

Towards a safe and efficient clinical implementation of machine learning in radiation oncology by exploring model interpretability, explainability and data-model dependency
- PMID: 35421855
- PMCID: PMC9870296
- DOI: 10.1088/1361-6560/ac678a
Towards a safe and efficient clinical implementation of machine learning in radiation oncology by exploring model interpretability, explainability and data-model dependency
Abstract
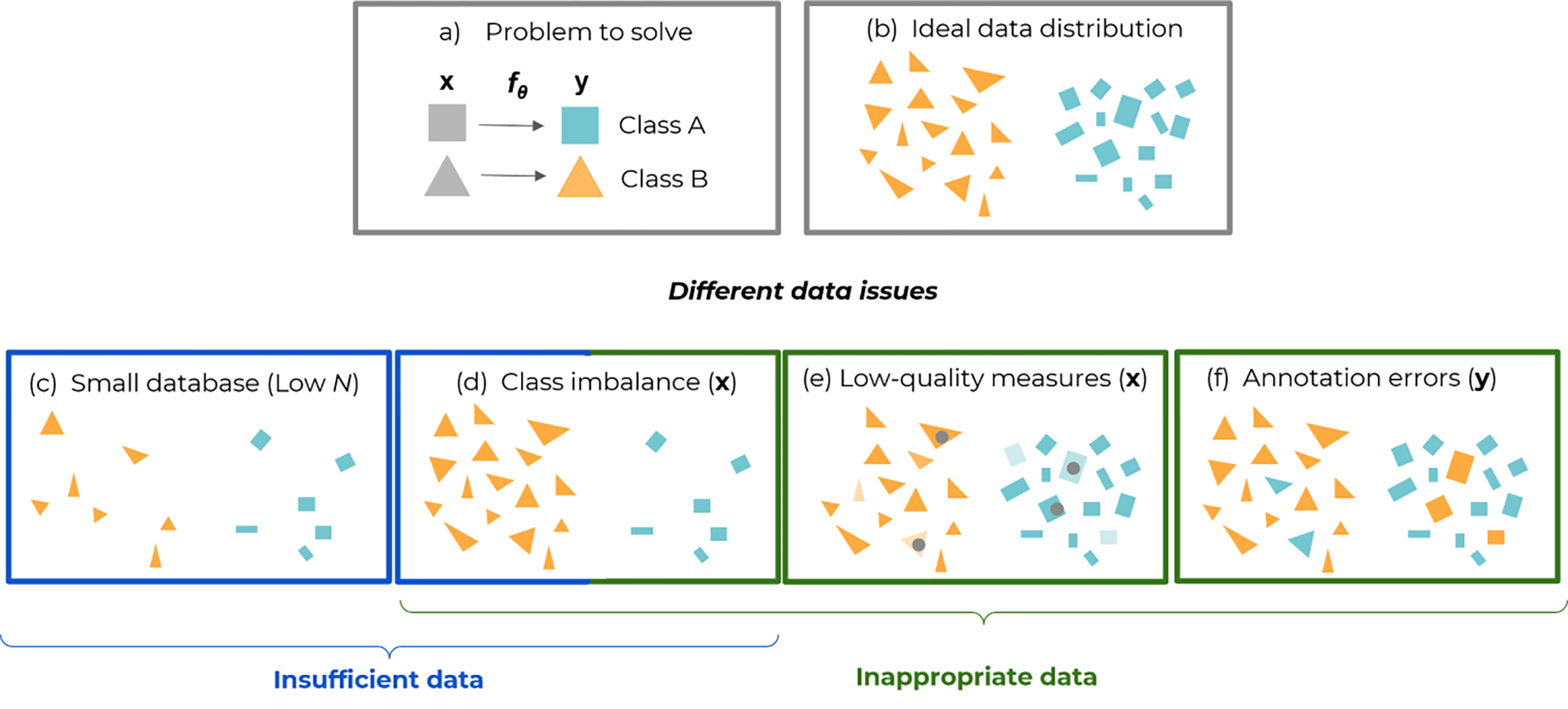
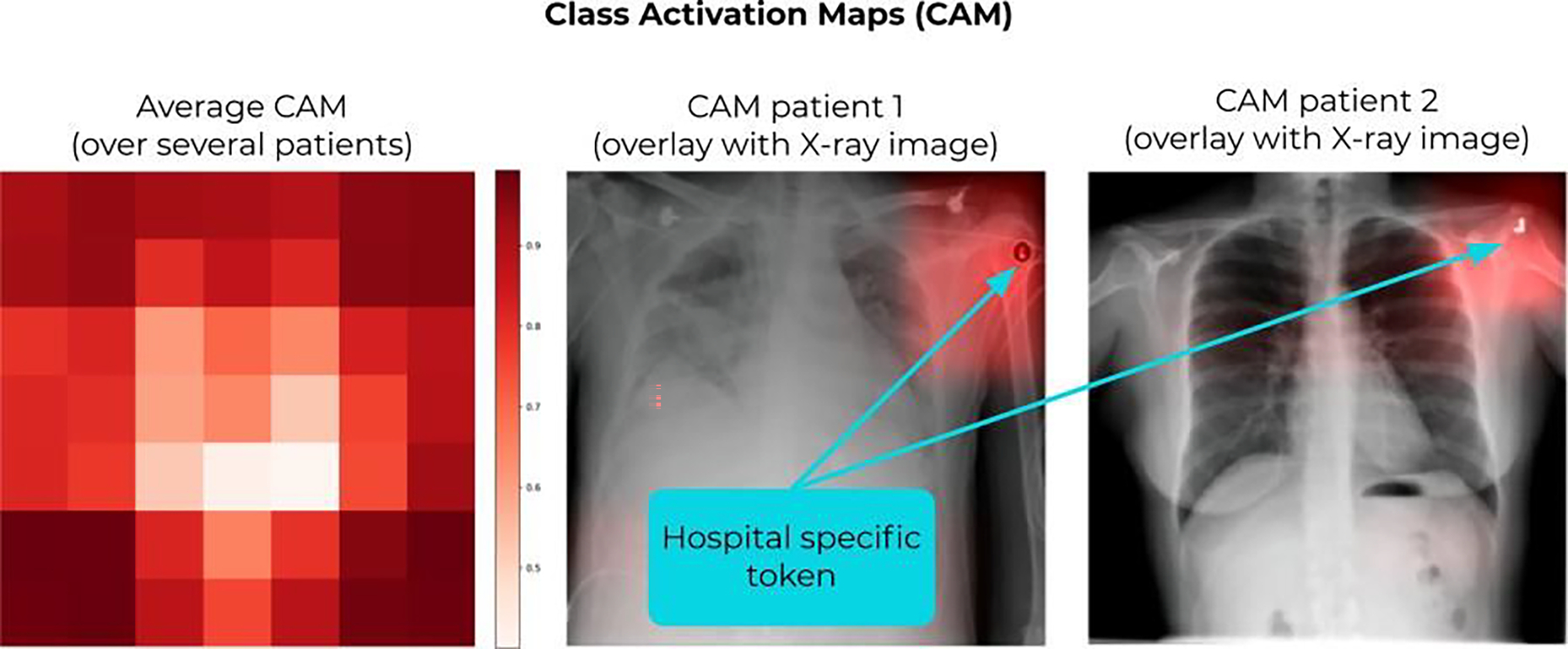
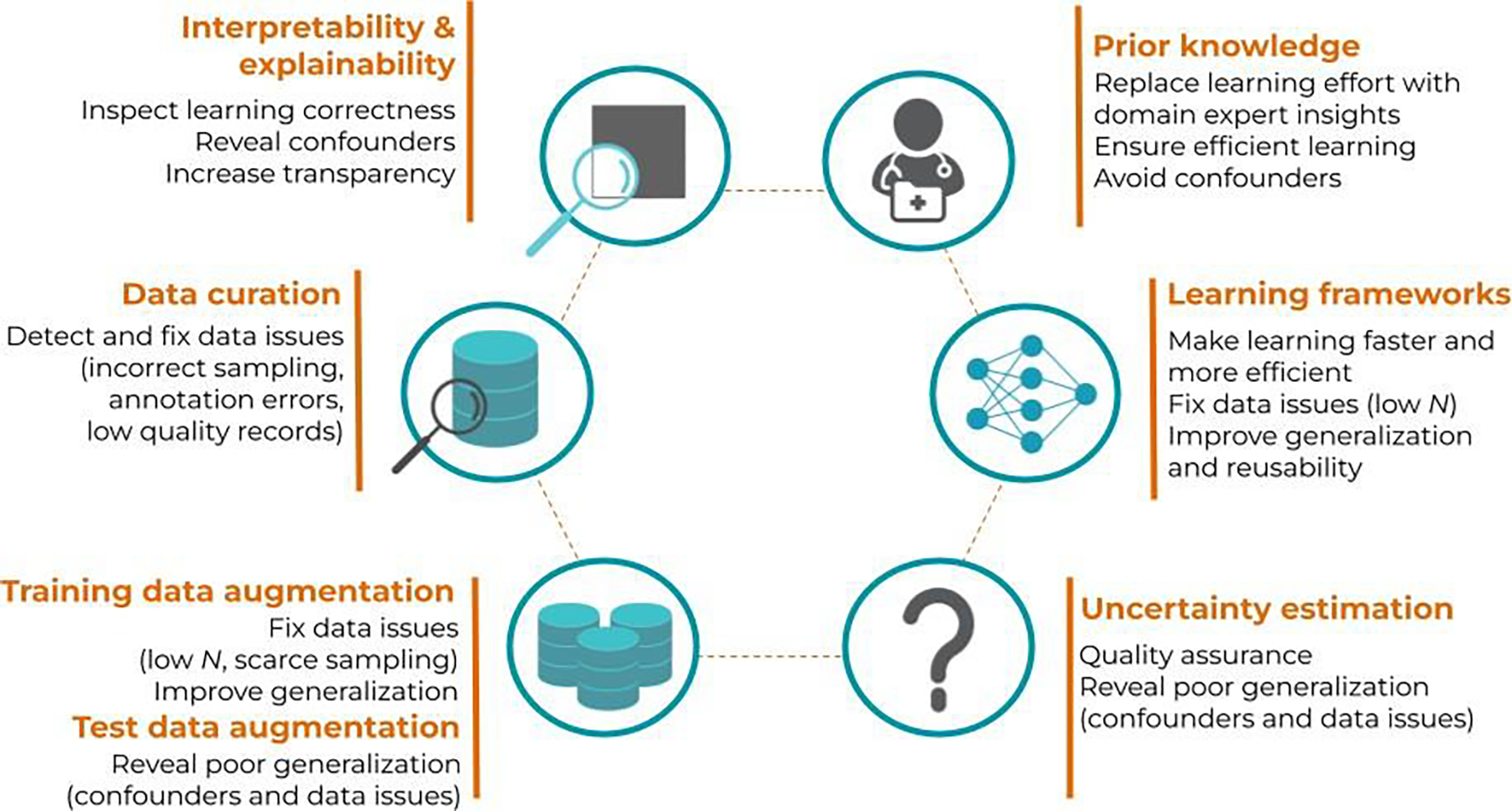
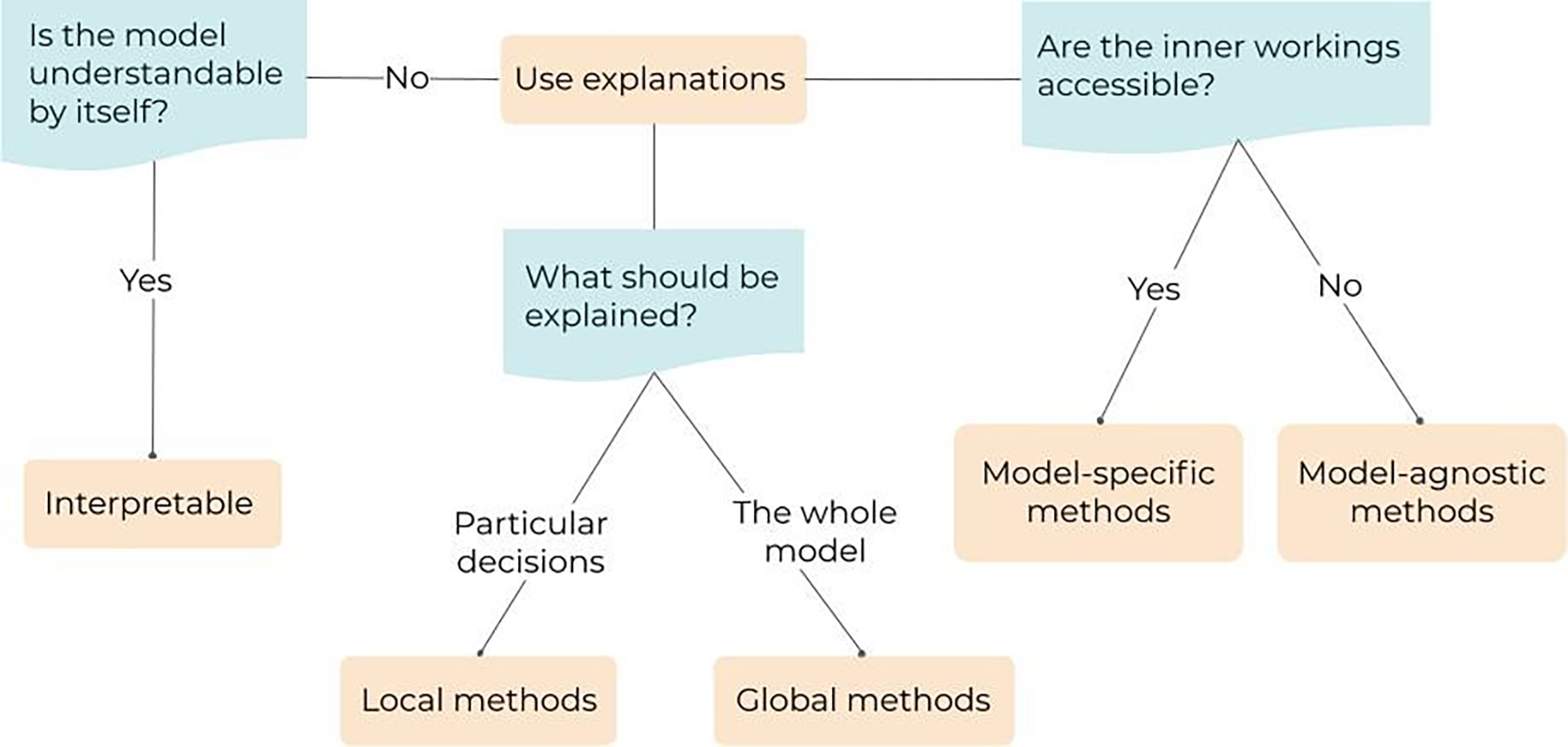
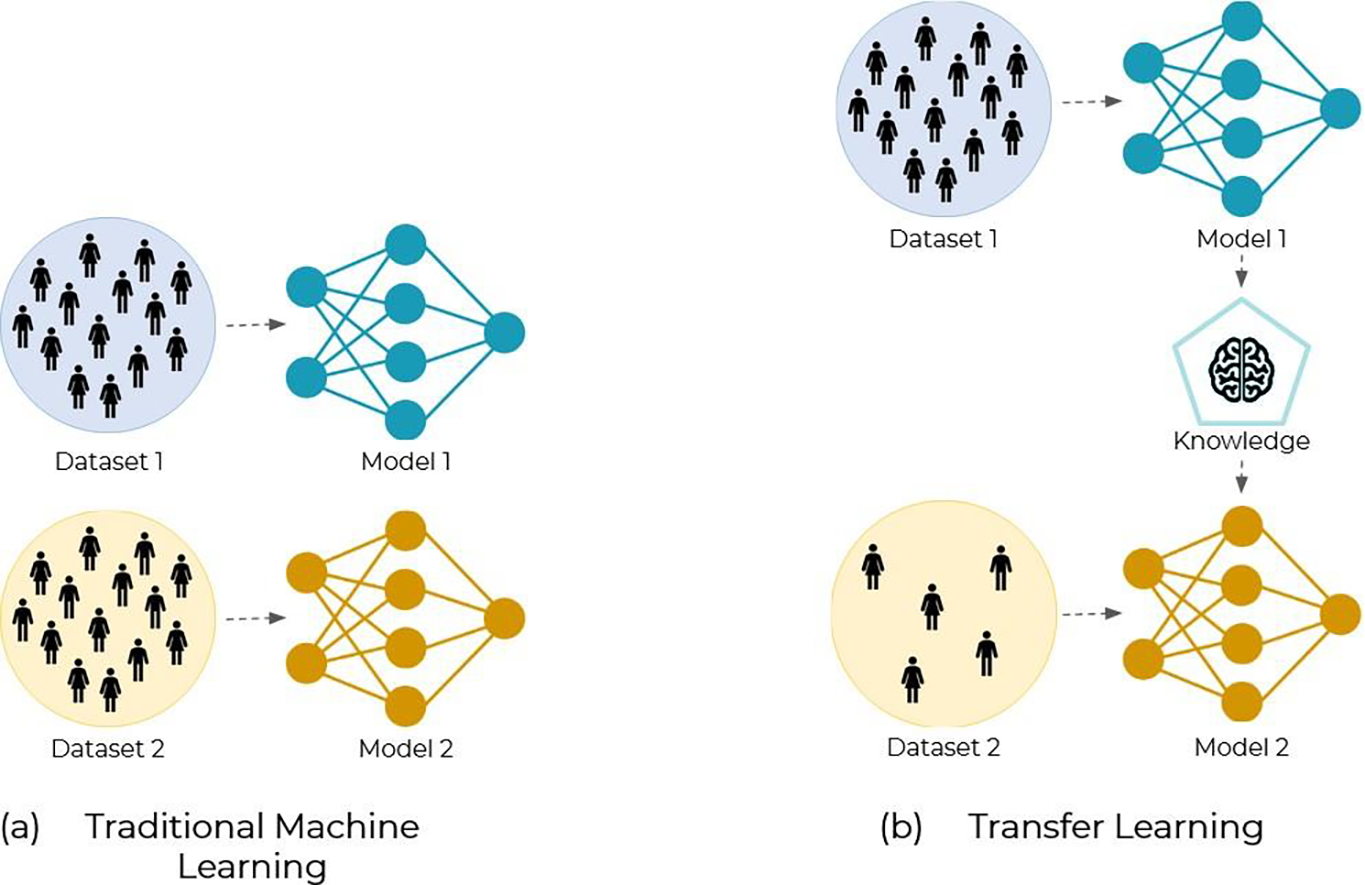
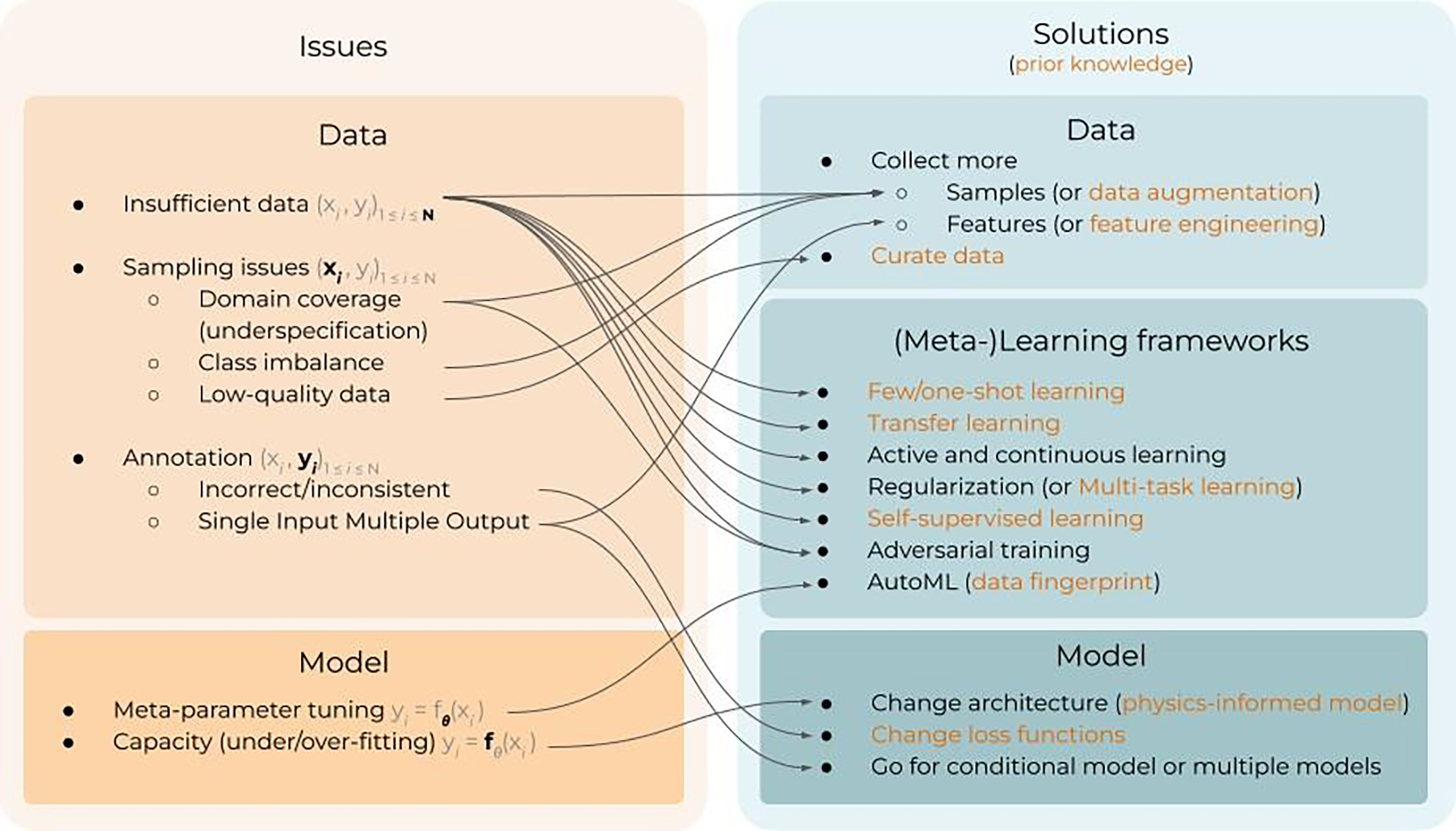
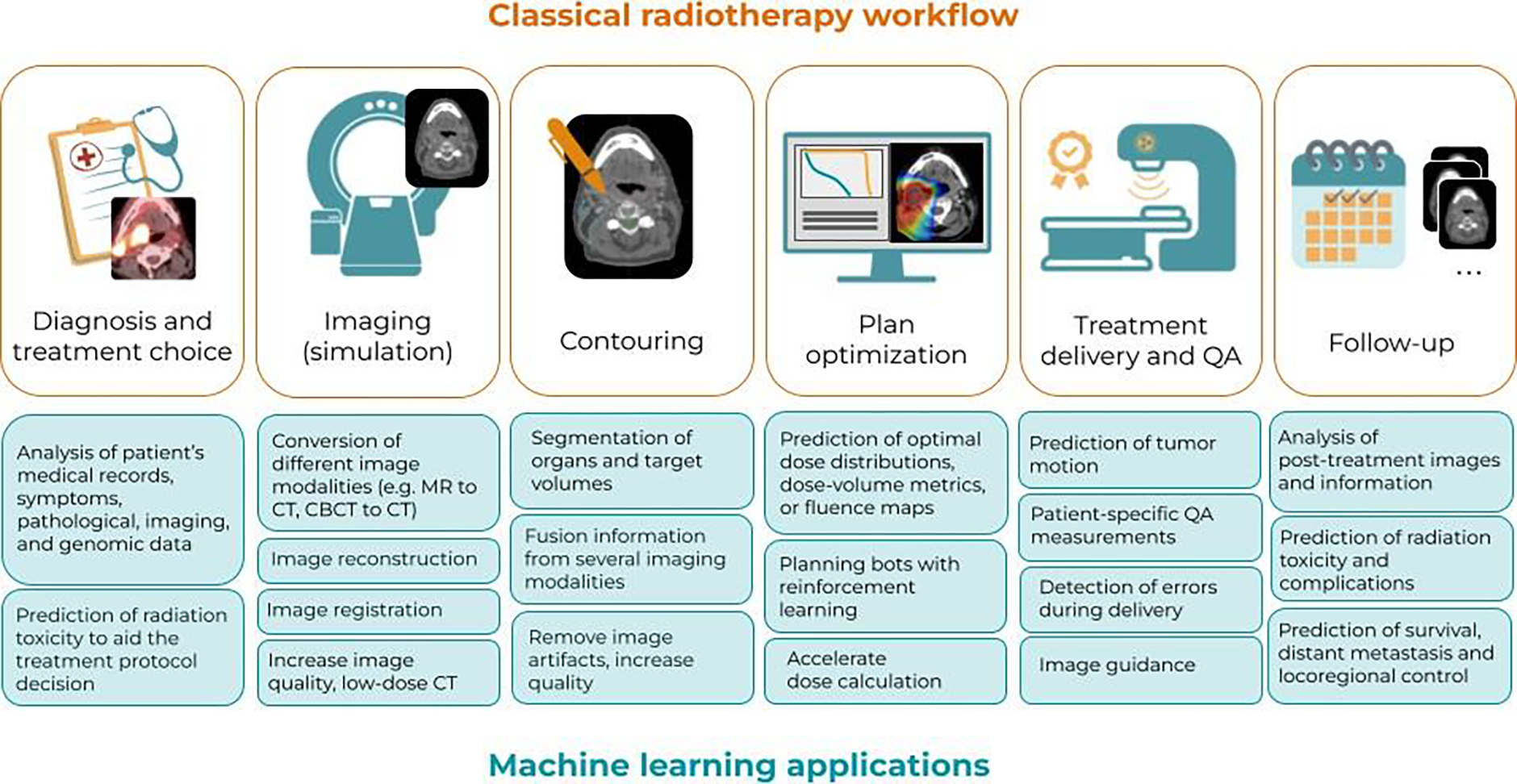
The interest in machine learning (ML) has grown tremendously in recent years, partly due to the performance leap that occurred with new techniques of deep learning, convolutional neural networks for images, increased computational power, and wider availability of large datasets. Most fields of medicine follow that popular trend and, notably, radiation oncology is one of those that are at the forefront, with already a long tradition in using digital images and fully computerized workflows. ML models are driven by data, and in contrast with many statistical or physical models, they can be very large and complex, with countless generic parameters. This inevitably raises two questions, namely, the tight dependence between the models and the datasets that feed them, and the interpretability of the models, which scales with its complexity. Any problems in the data used to train the model will be later reflected in their performance. This, together with the low interpretability of ML models, makes their implementation into the clinical workflow particularly difficult. Building tools for risk assessment and quality assurance of ML models must involve then two main points: interpretability and data-model dependency. After a joint introduction of both radiation oncology and ML, this paper reviews the main risks and current solutions when applying the latter to workflows in the former. Risks associated with data and models, as well as their interaction, are detailed. Next, the core concepts of interpretability, explainability, and data-model dependency are formally defined and illustrated with examples. Afterwards, a broad discussion goes through key applications of ML in workflows of radiation oncology as well as vendors' perspectives for the clinical implementation of ML.
Keywords: clinical implementation; interpretability and explainability; machine learning; radiation oncology; uncertainty quantification.
Creative Commons Attribution license.
Figures
References
-
- Abdar M, Pourpanah F, Hussain S, Rezazadegan D, Liu L, Ghavamzadeh M, Fieguth P, Cao X, Khosravi A, Rajendra Acharya U, Makarenkov V and Nahavandi S 2021. A review of uncertainty quantification in deep learning: Techniques, applications and challenges Information Fusion 76 243–97 Online: 10.1016/j.inffus.2021.05.008 - DOI
-
- Adadi A and Berrada M 2018. Peeking Inside the Black-Box: A Survey on Explainable Artificial Intelligence (XAI) IEEE Access 6 52138–60 Online: 10.1109/access.2018.2870052 - DOI
-
- Ahishakiye E, Van Gijzen M B, Tumwiine J, Wario R and Obungoloch J 2021. A survey on deep learning in medical image reconstruction Intelligent Medicine 1 118–27 Online: 10.1016/j.imed.2021.03.003 - DOI