

Comparing prevalence of chronic kidney disease and its risk factors between population-based surveys in Russia and Norway
- PMID: 35421937
- PMCID: PMC9008943
- DOI: 10.1186/s12882-022-02738-2
Comparing prevalence of chronic kidney disease and its risk factors between population-based surveys in Russia and Norway
Abstract
Background: Little data exists on the prevalence of chronic kidney disease (CKD) in the Russian population. We aimed to estimate the prevalence of CKD in a population-based study in Russia, compare with a similar study in Norway, and investigate whether differences in risk factors explained between-study differences in CKD.
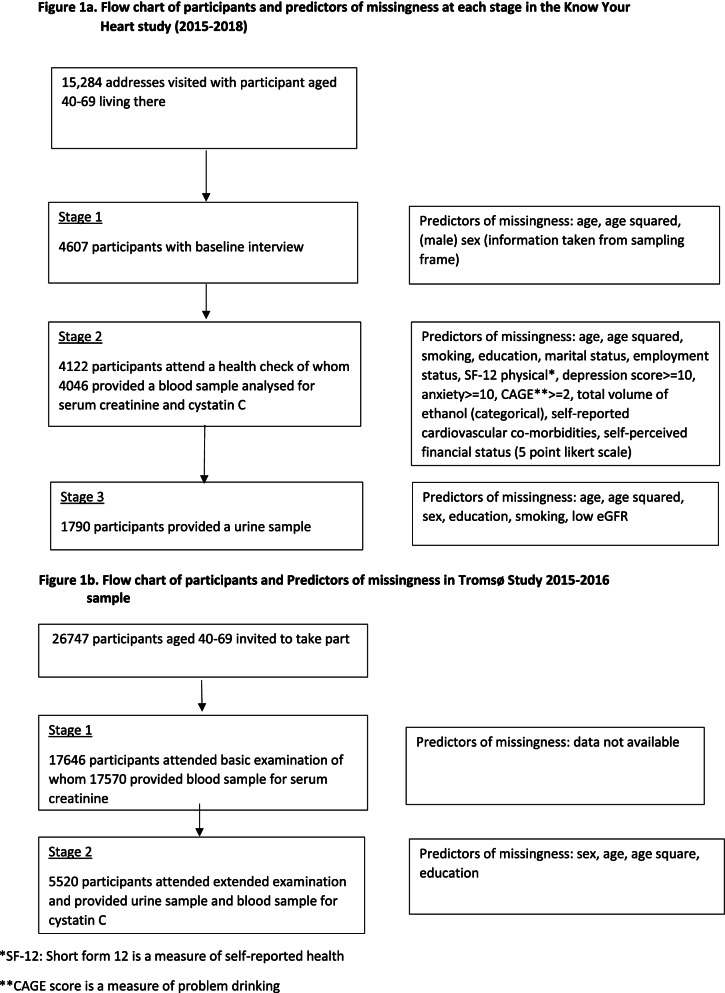
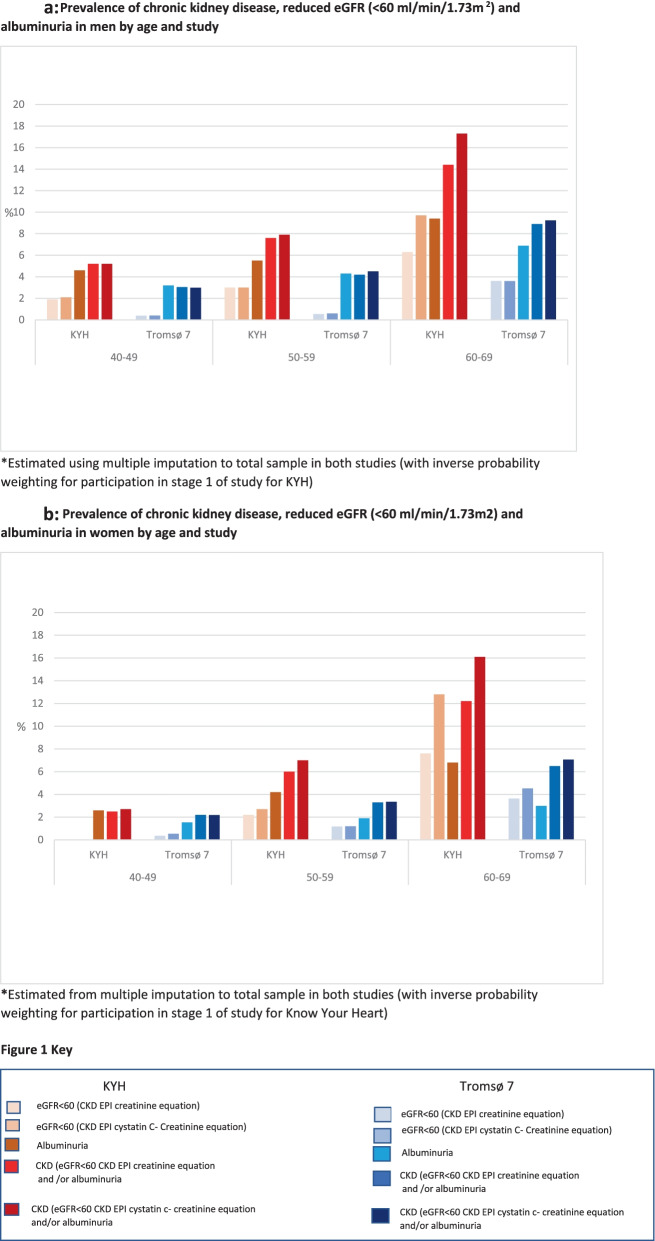
Methods: We compared age- and sex-standardised prevalence of reduced eGFR (< 60 ml/min/1.73m2 CKD-EPI creatinine equation), albuminuria and or a composite indicator of CKD (one measure of either reduced eGFR or albuminuria) between participants aged 40-69 in the population-based Know Your Heart (KYH) study, Russia (2015-2018 N = 4607) and the seventh Tromsø Study (Tromsø7), Norway (2015-2016 N = 17,646). We assessed the contribution of established CKD risk factors (low education, diabetes, hypertension, antihypertensive use, smoking, obesity) to between-study differences using logistic regression.
Results: Prevalence of reduced eGFR or albuminuria was 6.5% (95% Confidence Interval (CI) 5.4, 7.7) in KYH and 4.6% (95% CI 4.0, 5.2) in Tromsø7 standardised for sex and age. Odds of both clinical outcomes were higher in KYH than Tromsø7 (reduced eGFR OR 2.06 95% CI 1.67, 2.54; albuminuria OR 1.54 95% CI 1.16, 2.03) adjusted for sex and age. Risk factor adjustment explained the observed between-study difference in albuminuria (OR 0.92 95% CI 0.68, 1.25) but only partially reduced eGFR (OR 1.42 95% CI 1.11, 1.82). The strongest explanatory factors for the between-study difference was higher use of antihypertensives (Russian sample) for reduced eGFR and mean diastolic blood pressure for albuminuria.
Conclusions: We found evidence of a higher burden of CKD within the sample from the population in Arkhangelsk and Novosibirsk compared to Tromsø, partly explained by between-study population differences in established risk factors. In particular hypertension defined by medication use was an important factor associated with the higher CKD prevalence in the Russian sample.
Keywords: Chronic kidney disease; Epidemiology; Norway; Risk factors; Russian Federation.
© 2022. The Author(s).
Conflict of interest statement
DN has received funding for two GSK funded studies looking at aspects of kidney function in children and adults in Sub-Saharan Africa in the past 36 months and is the UK Renal Association Director of Informatics Research. DAL declares institutional payment for consultancy work providing expert advice on determinants of longevity as a member of a scientific panel. EW has received payments from AZ for providing statistical training, unrelated to the submitted work. SM and AR are supported by Russian Academy of Science (State assignment АААА-А17–117112850280-2). SM declares additionally funding for equipment and travel as part of the International Project on Cardiovascular Disease in Russia (IPCDR) project funded by Wellcome Trust Strategic Award as detailed in funding statement. All other authors declare they have no conflicts of interest.
Figures
Similar articles
-
Uncontrolled and apparent treatment resistant hypertension: a cross-sectional study of Russian and Norwegian 40-69 year olds.BMC Cardiovasc Disord. 2020 Mar 13;20(1):135. doi: 10.1186/s12872-020-01407-2. BMC Cardiovasc Disord. 2020. PMID: 32169049 Free PMC article.
-
Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in a central Chinese urban population: a cross-sectional survey.BMC Nephrol. 2020 Apr 3;21(1):115. doi: 10.1186/s12882-020-01761-5. BMC Nephrol. 2020. PMID: 32245423 Free PMC article.
-
Chronic kidney disease in Russia: the Ural eye and medical study.BMC Nephrol. 2020 May 25;21(1):198. doi: 10.1186/s12882-020-01843-4. BMC Nephrol. 2020. PMID: 32450794 Free PMC article.
-
Prevalence and risk factors of chronic kidney disease in urban adult Cameroonians according to three common estimators of the glomerular filtration rate: a cross-sectional study.BMC Nephrol. 2015 Jul 7;16:96. doi: 10.1186/s12882-015-0102-9. BMC Nephrol. 2015. PMID: 26149764 Free PMC article.
-
The prevalence of chronic kidney disease in South Africa - limitations of studies comparing prevalence with sub-Saharan Africa, Africa, and globally.BMC Nephrol. 2023 Mar 21;24(1):62. doi: 10.1186/s12882-023-03109-1. BMC Nephrol. 2023. PMID: 36944928 Free PMC article.
Cited by
-
Global health inequalities of chronic kidney disease: a meta-analysis.Nephrol Dial Transplant. 2024 Sep 27;39(10):1692-1709. doi: 10.1093/ndt/gfae048. Nephrol Dial Transplant. 2024. PMID: 38389223 Free PMC article.
-
Waist-to-Height Ratio - Reference Values and Associations with Cardiovascular Risk Factors in a Russian Adult Population.Diabetes Metab Syndr Obes. 2025 Aug 1;18:2641-2653. doi: 10.2147/DMSO.S491261. eCollection 2025. Diabetes Metab Syndr Obes. 2025. PMID: 40771439 Free PMC article.
References
-
- Global Health Observatory. World Health Organisation. Total NCD Mortality Data by country. 2017. Geneva: Available online http://apps.who.int/gho/data/node.main.A860?lang=en. [cited 2018 08/05/18].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
