

Ranked determinants of telemedicine diabetic retinopathy screening performance in the United States primary care safety-net setting: an exploratory CART analysis
- PMID: 35421978
- PMCID: PMC9011929
- DOI: 10.1186/s12913-022-07915-5
Ranked determinants of telemedicine diabetic retinopathy screening performance in the United States primary care safety-net setting: an exploratory CART analysis
Abstract
Background: Diabetic retinopathy (DR) is a leading cause of blindness worldwide, despite easy detection and effective treatment. Annual screening rates in the USA remain low, especially for the disadvantaged, which telemedicine-based DR screening (TDRS) during routine primary care has been shown to improve. Screening rates from such programs have varied, however, pointing to inconsistent implementation and unaddressed barriers. This work seeks to identify and prioritize modifiable barriers for targeted intervention.
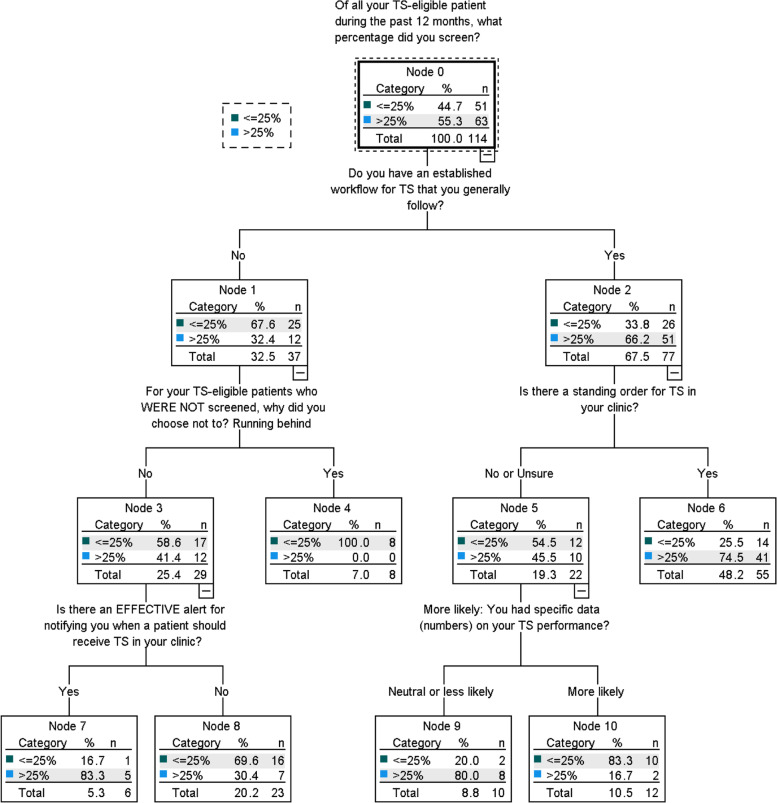
Methods: In this final phase of an exploratory mixed-methods study, we developed, validated, and administered a 62-item survey to multilevel stakeholders involved with TDRS in primary care safety-net clinics. Survey items were aligned with previously identified determinants of clinic-level screening and mapped to the Consolidated Framework for Implementation Research (CFIR). Classification and Regression Tree (CART) analyses were used to identify and rank independent variables predictive of individual-level TDRS screening performance.
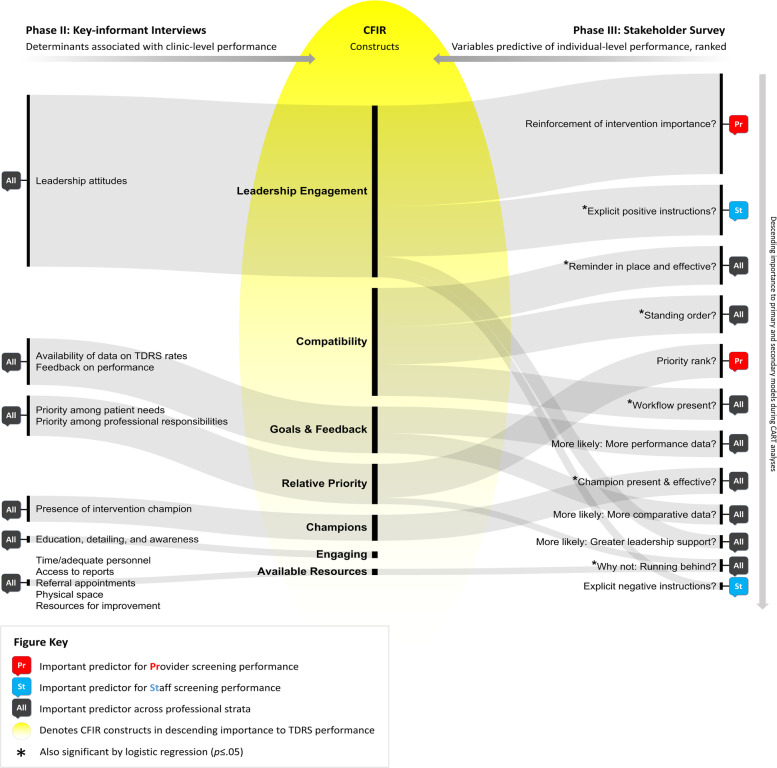
Results: Overall, 133 of the 341 invited professionals responded (39%), representing 20 safety-net clinics across 6 clinical systems. Respondents were predominately non-Hispanic White (77%), female (94%), and between 31 and 65 years of age (79%). Satisfaction with TDRS was high despite low self-reported screening rates. The most important screening determinants were: provider reinforcement of TDRS importance; explicit instructions by providers to staff; effective reminders; standing orders; high relative priority among routine diabetic measures; established TDRS workflows; performance feedback; effective TDRS champions; and leadership support.
Conclusions: In this survey of stakeholders involved with TDRS in safety-net clinics, screening was low despite high satisfaction with the intervention. The best predictors of screening performance mapped to the CFIR constructs Leadership Engagement, Compatibility, Goals & Feedback, Relative Priority, Champions, and Available Resources. These findings facilitate the prioritization of implementation strategies targeting determinants of TDRS performance, potentially increasing its public health impact.
Keywords: Barriers and facilitators; Classification and regression tree (CART); Consolidated framework for implementation research (CFIR); Determinants; Diabetic retinopathy; Mixed methods; Primary care; Screening; Telemedicine; Underserved.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Comprehensive Diabetes Care. NCQA. https://www.ncqa.org/hedis/measures/comprehensive-diabetes-care/. Accessed 18 Mar 2020.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
