

Rapidly improving acute respiratory distress syndrome in COVID-19: a multi-centre observational study
- PMID: 35422037
- PMCID: PMC9008400
- DOI: 10.1186/s12931-022-02015-8
Rapidly improving acute respiratory distress syndrome in COVID-19: a multi-centre observational study
Abstract
Background: Before the pandemic of coronavirus disease (COVID-19), rapidly improving acute respiratory distress syndrome (ARDS), mostly defined by early extubation, had been recognized as an increasingly prevalent subphenotype (making up 15-24% of all ARDS cases), associated with good prognosis (10% mortality in ARDSNet trials). We attempted to determine the prevalence and prognosis of rapidly improving ARDS and of persistent severe ARDS related to COVID-19.
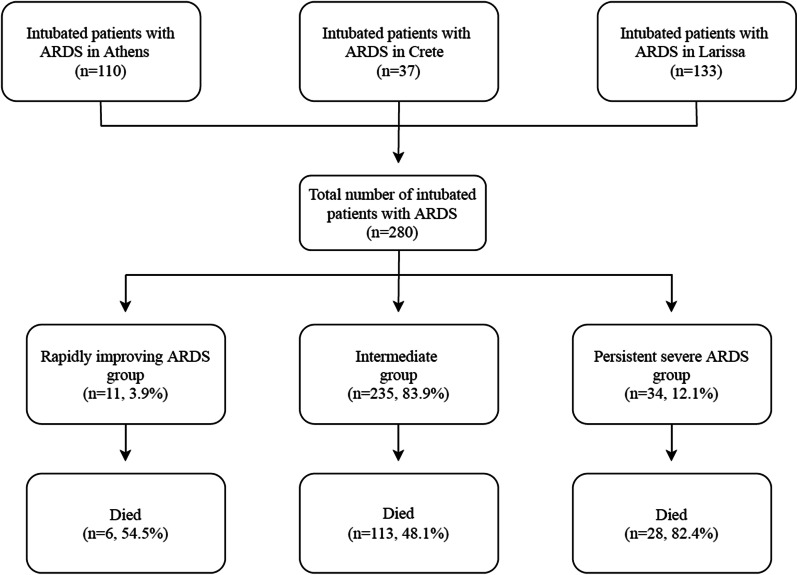
Methods: We included consecutive patients with COVID-19 receiving invasive mechanical ventilation in three intensive care units (ICU) during the second pandemic wave in Greece. We defined rapidly improving ARDS as extubation or a partial pressure of arterial oxygen to fraction of inspired oxygen ratio (PaO2:FiO2) greater than 300 on the first day following intubation. We defined persistent severe ARDS as PaO2:FiO2 of equal to or less than 100 on the second day following intubation.
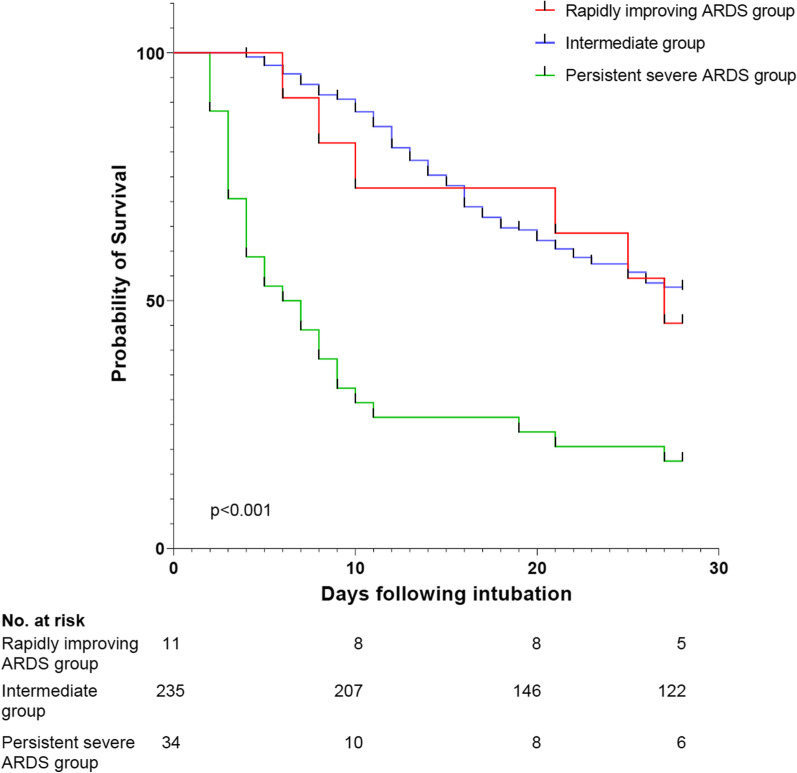
Results: A total of 280 intubated patients met criteria of ARDS with a median PaO2:FiO2 of 125.0 (interquartile range 93.0-161.0) on day of intubation, and overall ICU-mortality of 52.5% (ranging from 24.3 to 66.9% across the three participating sites). Prevalence of rapidly improving ARDS was 3.9% (11 of 280 patients); no extubation occurred on the first day following intubation. ICU-mortality of patients with rapidly improving ARDS was 54.5%. This low prevalence and high mortality rate of rapidly improving ARDS were consistent across participating sites. Prevalence of persistent severe ARDS was 12.1% and corresponding mortality was 82.4%.
Conclusions: Rapidly improving ARDS was not prevalent and was not associated with good prognosis among patients with COVID-19. This is starkly different from what has been previously reported for patients with ARDS not related to COVID-19. Our results on both rapidly improving ARDS and persistent severe ARDS may contribute to our understanding of trajectory of ARDS and its association with prognosis in patients with COVID-19.
Keywords: Acute respiratory distress syndrome; Acute respiratory failure; Coronavirus; Pneumonia; Trajectory.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. IIS serves as Associate Editor for the Journal.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
