

Drinking water chlorination has minor effects on the intestinal flora and resistomes of Bangladeshi children
- PMID: 35422497
- PMCID: PMC9249080
- DOI: 10.1038/s41564-022-01101-3
Drinking water chlorination has minor effects on the intestinal flora and resistomes of Bangladeshi children
Abstract
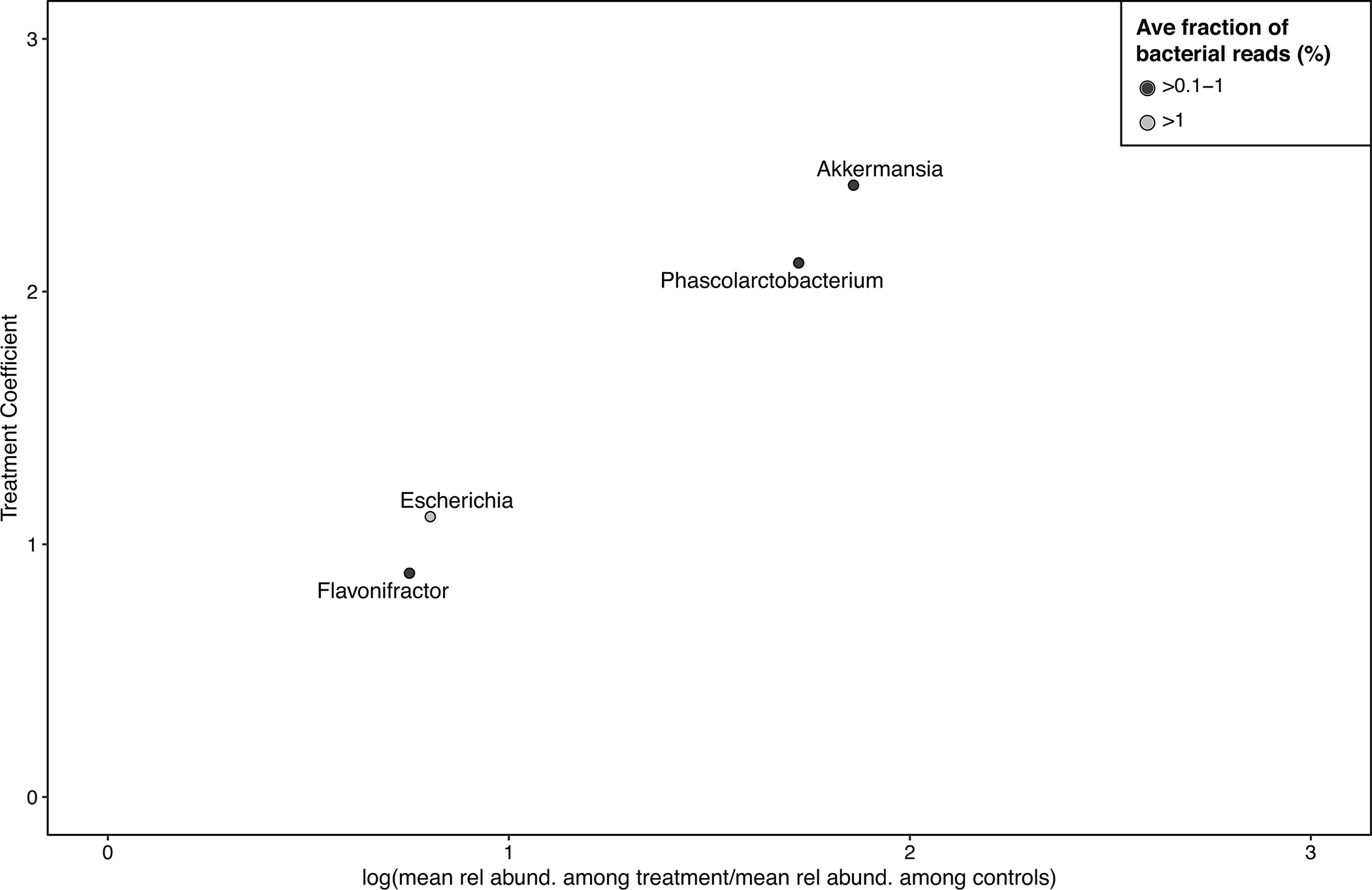
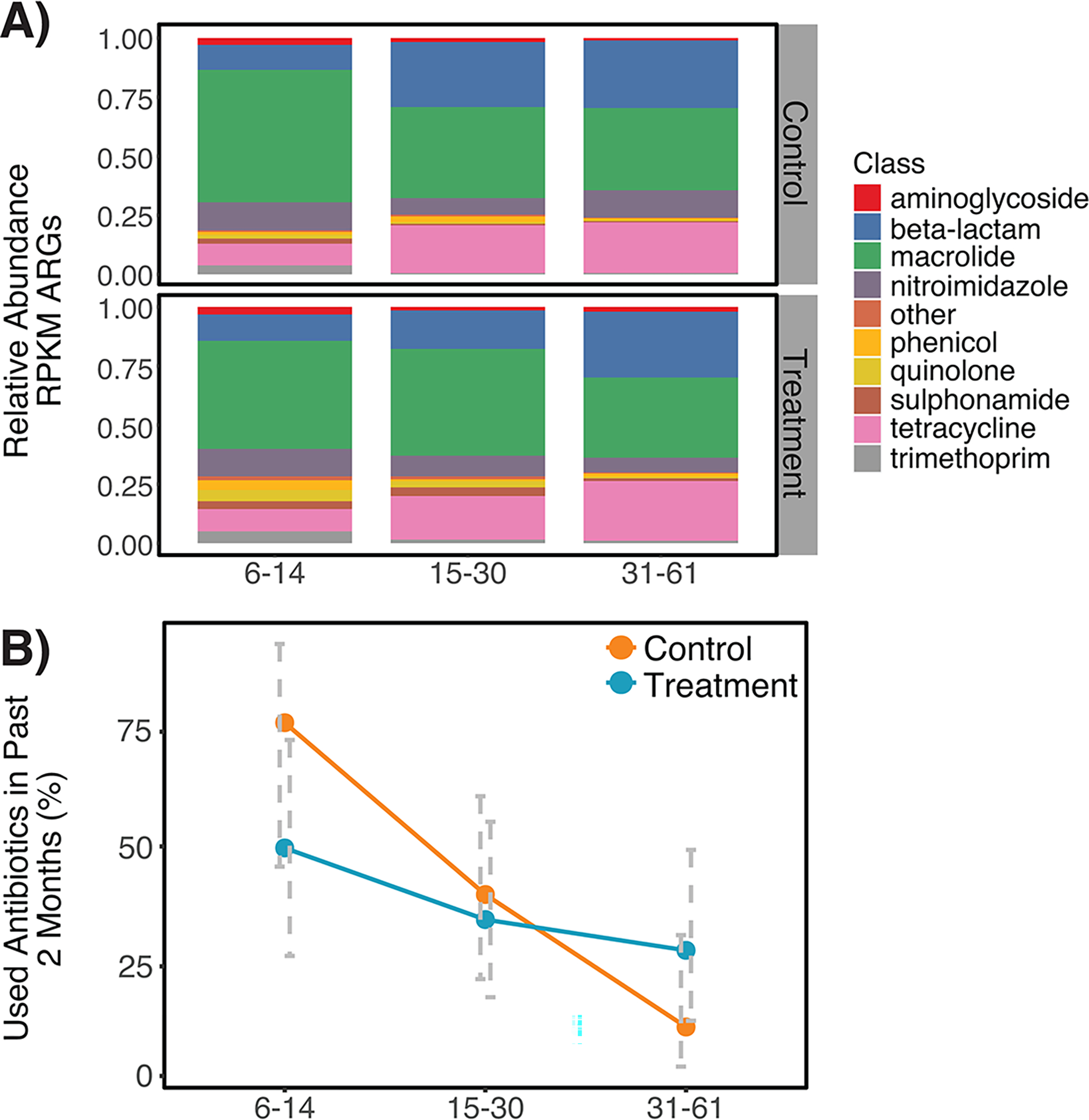
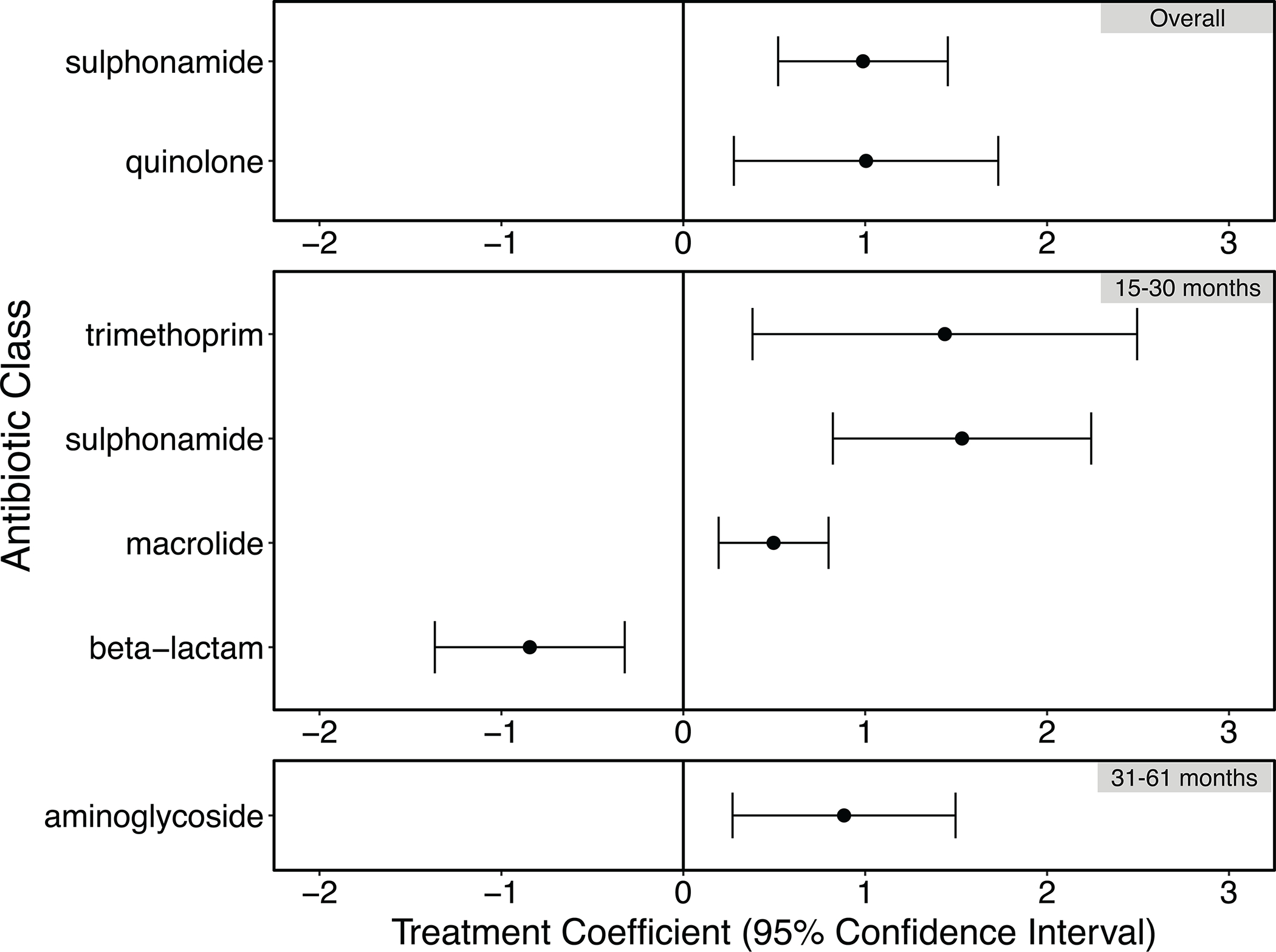
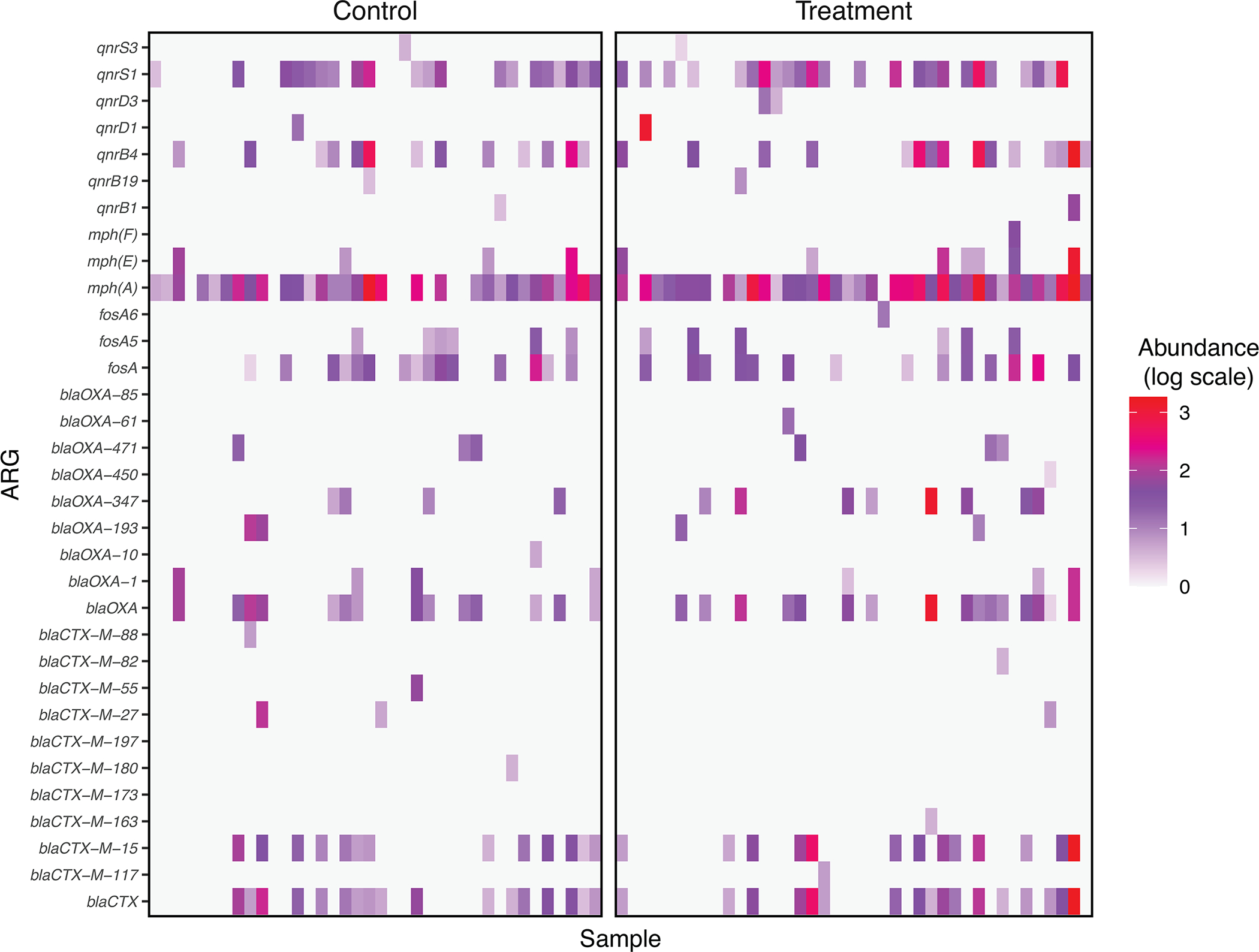
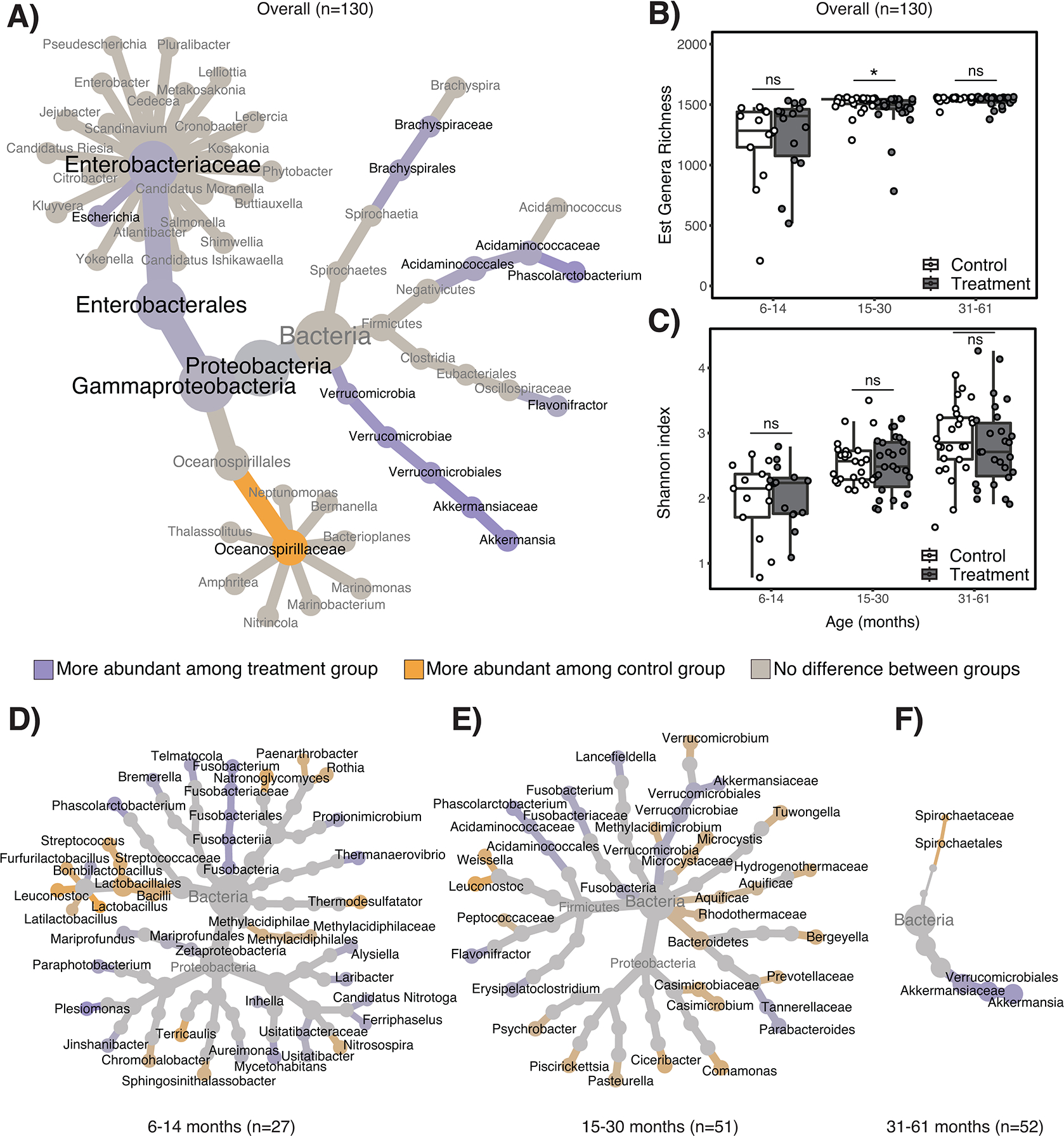
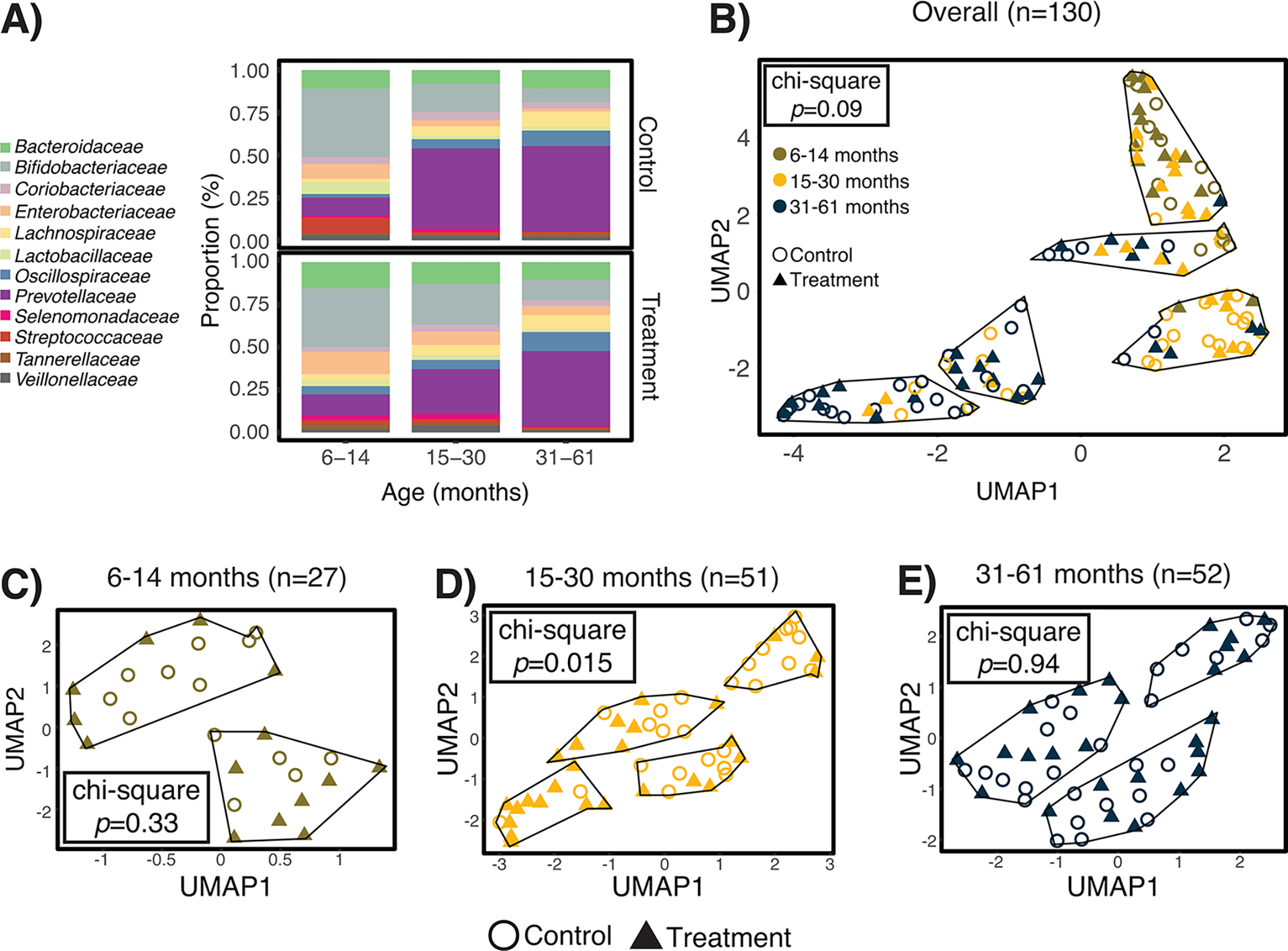
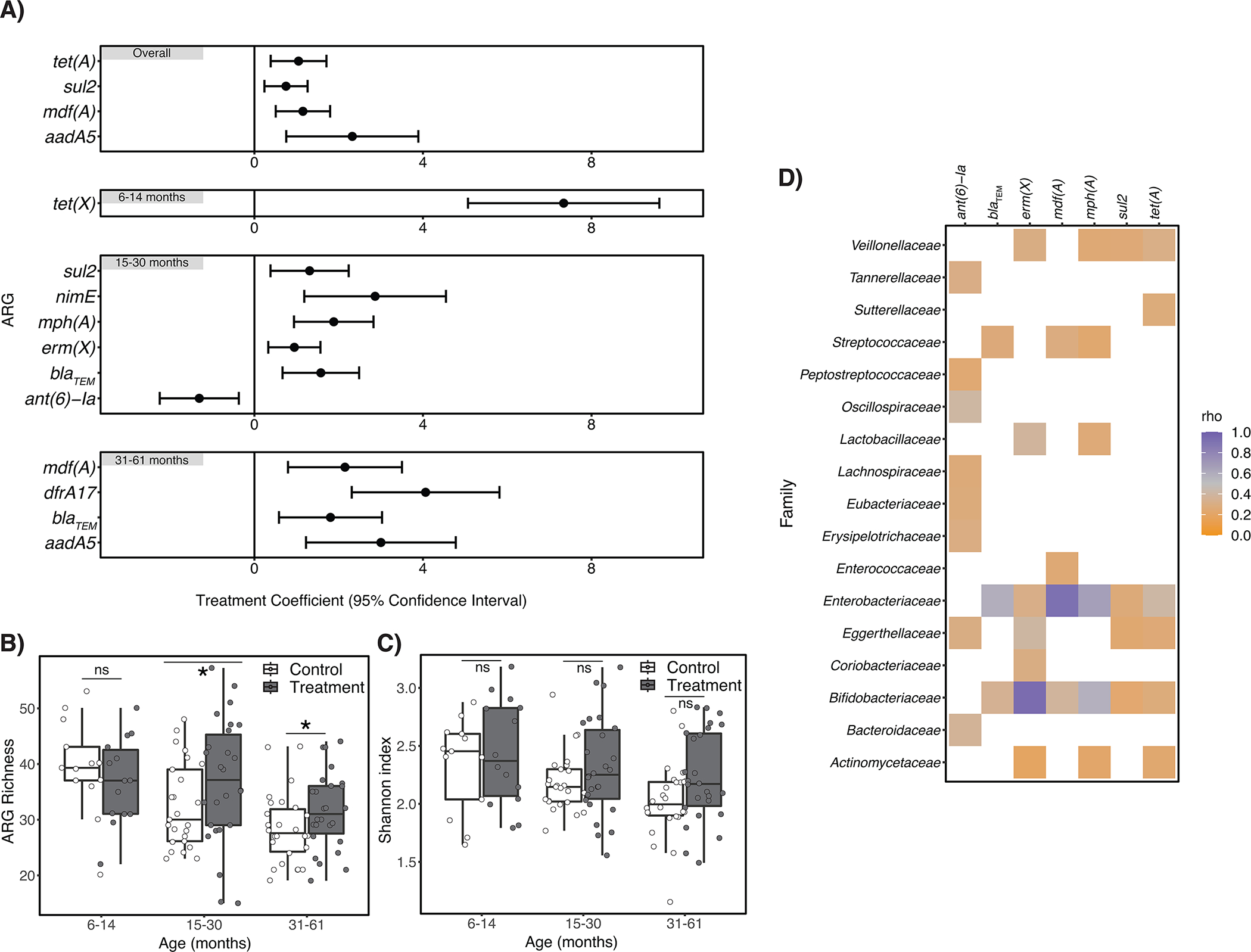
Healthy development of the gut microbiome provides long-term health benefits. Children raised in countries with high infectious disease burdens are frequently exposed to diarrhoeal pathogens and antibiotics, which perturb gut microbiome assembly. A recent cluster-randomized trial leveraging >4,000 child observations in Dhaka, Bangladesh, found that automated water chlorination of shared taps effectively reduced child diarrhoea and antibiotic use. In this substudy, we leveraged stool samples collected from 130 children 1 year after chlorine doser installation to examine differences between treatment and control children's gut microbiota. Water chlorination was associated with increased abundance of several bacterial genera previously linked to improved gut health; however, we observed no effects on the overall richness or diversity of taxa. Several clinically relevant antibiotic resistance genes were relatively more abundant in the gut microbiome of treatment children, possibly due to increases in Enterobacteriaceae. While further studies on the long-term health impacts of drinking chlorinated water would be valuable, we conclude that access to chlorinated water did not substantially impact child gut microbiome development in this setting, supporting the use of chlorination to increase global access to safe drinking water.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Competing interests statement
The authors report no relevant financial or non-financial competing interests.
Figures
References
-
- Robertson RC, Manges AR, Finlay BB & Prendergast AJ The Human Microbiome and Child Growth – First 1000 Days and Beyond. Trends in Microbiology 27, 131–147 (2019). - PubMed
