

Neutrophil inhibition improves acute inflammation in a murine model of viral myocarditis
- PMID: 35426438
- PMCID: PMC9847559
- DOI: 10.1093/cvr/cvac052
Neutrophil inhibition improves acute inflammation in a murine model of viral myocarditis
Abstract
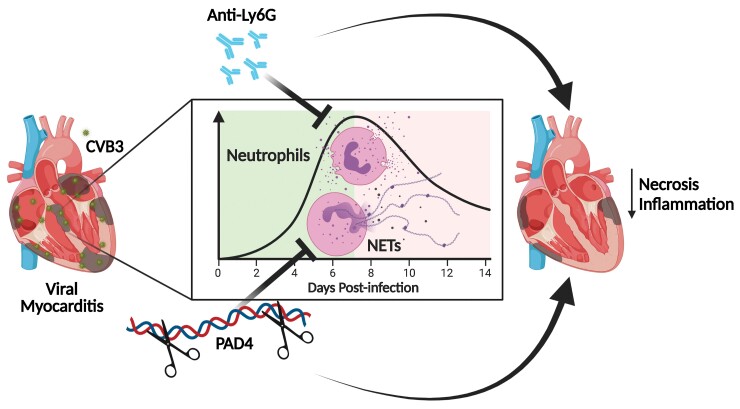
Aims: Viral myocarditis (VM) is an inflammatory pathology of the myocardium triggered by a viral infection that may cause sudden death or heart failure (HF), especially in the younger population. Current treatments only stabilize and improve cardiac function without resolving the underlying inflammatory cause. The factors that induce VM to progress to HF are still uncertain, but neutrophils have been increasingly associated with the negative evolution of cardiac pathologies. The present study investigates the contribution of neutrophils to VM disease progression in different ways.
Methods and results: In a coxsackievirus B3- (CVB3) induced mouse model of VM, neutrophils and neutrophil extracellular traps (NETs) were prominent in the acute phase of VM as revealed by enzyme-linked immunosorbent assay analysis and immunostaining. Anti-Ly6G-mediated neutrophil blockade starting at model induction decreased cardiac necrosis and leucocyte infiltration, preventing monocyte and Ly6CHigh pro-inflammatory macrophage recruitment. Furthermore, genetic peptidylarginine deiminase 4-dependent NET blockade reduced cardiac damage and leucocyte recruitment, significantly decreasing cardiac monocyte and macrophage presence. Depleting neutrophils with anti-Ly6G antibodies at 7 days post-infection, after the acute phase, did not decrease cardiac inflammation.
Conclusion: Collectively, these results indicate that the repression of neutrophils and the related NET response in the acute phase of VM improves the pathological phenotype by reducing cardiac inflammation.
Keywords: Coxsackievirus B3; Inflammation; Neutrophil extracellular traps; Neutrophils; Viral myocarditis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: S.H. receives personal fees for scientific advice to Astra-Zeneca, Cellprothera, CSL Behring, and Merck; unrestricted research grant from Pfizer. K.M. has received consulting fees for scientific advice to PEEL Therapeutics. All the remaining authors, P.C., L.F.G., S.V.B., V.S., D.D.G., N.G., and E.A.V.J., declare no competing interests.
Figures





References
-
- Weintraub RG, Semsarian C, Macdonald P. Dilated cardiomyopathy. Lancet 2017;390:400–414. - PubMed
-
- Tschöpe C, Ammirati E, Bozkurt B, Caforio ALP, Cooper LT, Felix SB, Hare JM, Heidecker B, Heymans S, Hübner N, Kelle S, Klingel K, Maatz H, Parwani AS, Spillmann F, Starling RC, Tsutsui H, Seferovic P, van Linthout S. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat Rev Cardiol 2021;18:169–193. - PMC - PubMed
-
- Corsten MF, Schroen B, Heymans S. Inflammation in viral myocarditis: friend or foe? Trends Mol Med 2012;18:426–437. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola V-P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. E Heart J 2016;37:2129–2200. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
