

Extending analytic methods for economic evaluation in implementation science
- PMID: 35428260
- PMCID: PMC9013084
- DOI: 10.1186/s13012-022-01192-w
Extending analytic methods for economic evaluation in implementation science
Abstract
Background: Economic evaluations of the implementation of health-related evidence-based interventions (EBIs) are conducted infrequently and, when performed, often use a limited set of quantitative methods to estimate the cost and effectiveness of EBIs. These studies often underestimate the resources required to implement and sustain EBIs in diverse populations and settings, in part due to inadequate scoping of EBI boundaries and underutilization of methods designed to understand the local context. We call for increased use of diverse methods, especially the integration of quantitative and qualitative approaches, for conducting and better using economic evaluations and related insights across all phases of implementation.
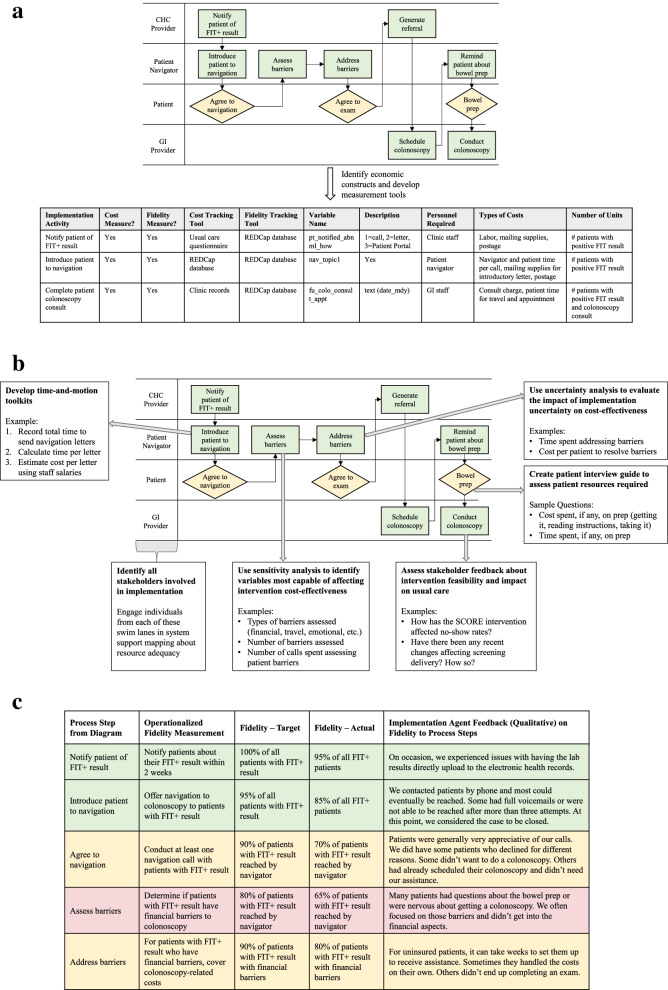
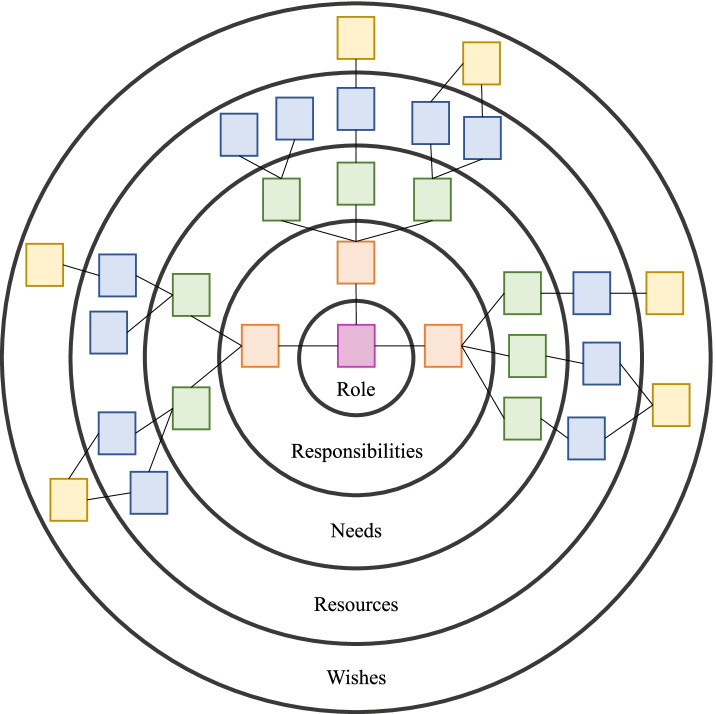
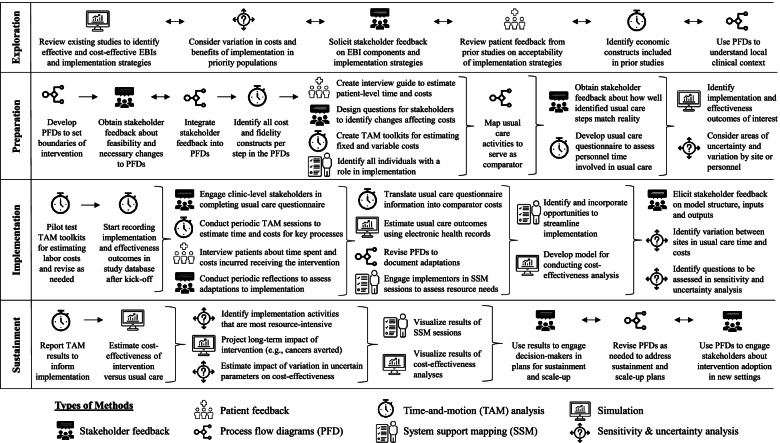
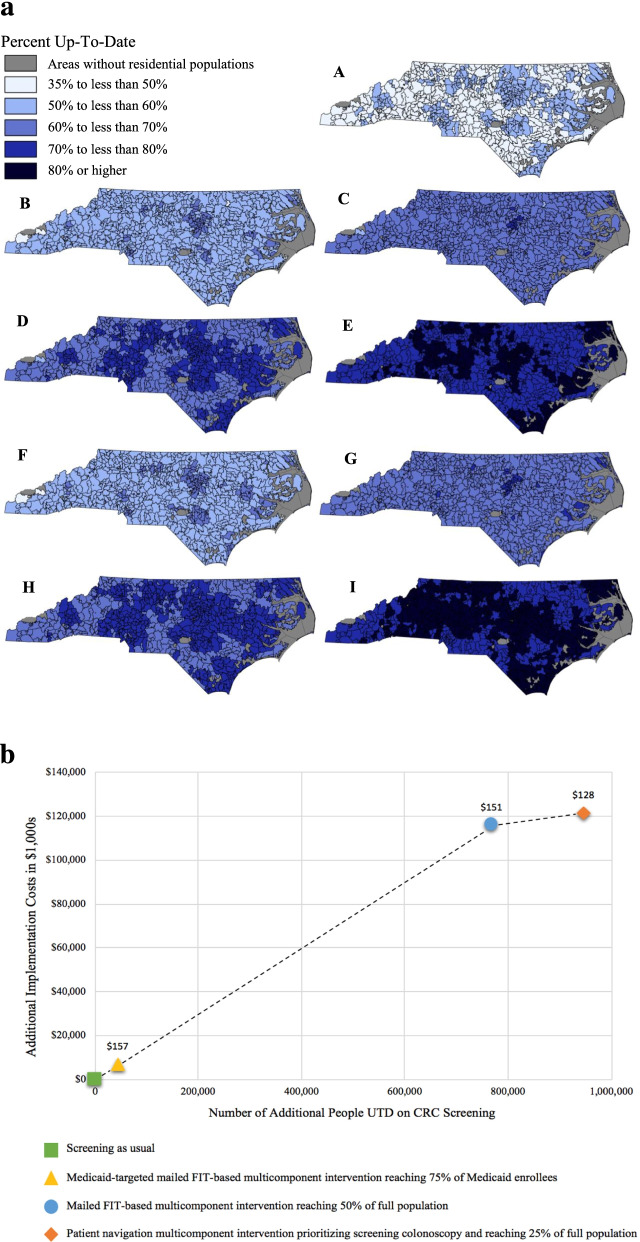
Main body: We describe methodological opportunities by implementation phase to develop more comprehensive and context-specific estimates of implementation costs and downstream impacts of EBI implementation, using the Exploration, Preparation, Implementation, Sustainment (EPIS) framework. We focus specifically on the implementation of complex interventions, which are often multi-level, resource-intensive, multicomponent, heterogeneous across sites and populations, involve many stakeholders and implementation agents, and change over time with respect to costs and outcomes. Using colorectal cancer (CRC) screening EBIs as examples, we outline several approaches to specifying the "boundaries" of EBI implementation and analyzing implementation costs by phase of implementation. We describe how systems mapping and stakeholder engagement methods can be used to clarify EBI implementation costs and guide data collection-particularly important when EBIs are complex. In addition, we discuss the use of simulation modeling with sensitivity/uncertainty analyses within implementation studies for projecting the health and economic impacts of investment in EBIs. Finally, we describe how these results, enhanced by careful data visualization, can inform selection, adoption, adaptation, and sustainment of EBIs.
Conclusion: Health economists and implementation scientists alike should draw from a larger menu of methods for estimating the costs and outcomes associated with complex EBI implementation and employ these methods across the EPIS phases. Our prior experiences using qualitative and systems approaches in addition to traditional quantitative methods provided rich data for informing decision-making about the value of investing in CRC screening EBIs and long-term planning for these health programs. Future work should consider additional opportunities for mixed-method approaches to economic evaluations.
Keywords: Colorectal cancer screening; Costs and cost analysis; Economic evaluation; Implementation science.
© 2022. The Author(s).
Conflict of interest statement
SBW receives funding paid to her institution from Pfizer Foundation and AstraZeneca for unrelated work. The other authors declare that they have no competing interests.
Figures
References
-
- Saldana L, Chamberlain P, Bradford WD, Campbell M, Landsverk J. The cost of implementing new strategies (COINS): a method for mapping implementation resources using the stages of implementation completion. Child Youth Serv Rev. 2014;39:177–182. doi: 10.1016/j.childyouth.2013.10.006. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
