

Sociodemographic characteristics and cervical cancer survival in different regions of the United States: a National Cancer Database study
- PMID: 35428687
- PMCID: PMC9177815
- DOI: 10.1136/ijgc-2021-003227
Sociodemographic characteristics and cervical cancer survival in different regions of the United States: a National Cancer Database study
Abstract
Objective: To determine how sociodemographic factors impact cervical cancer survival in different geographic locations in the USA.
Methods: A retrospective cohort of patients with cervical cancer from January 1, 2004 to December 31, 2015 in the National Cancer Database (NCDB) was identified. Tumor characteristics as well as race, income, insurance type, and treating facility types were compared among nine geographic regions. χ2 tests and Cox regression were used to compare differences between regions; p values <0.05 were considered significant.
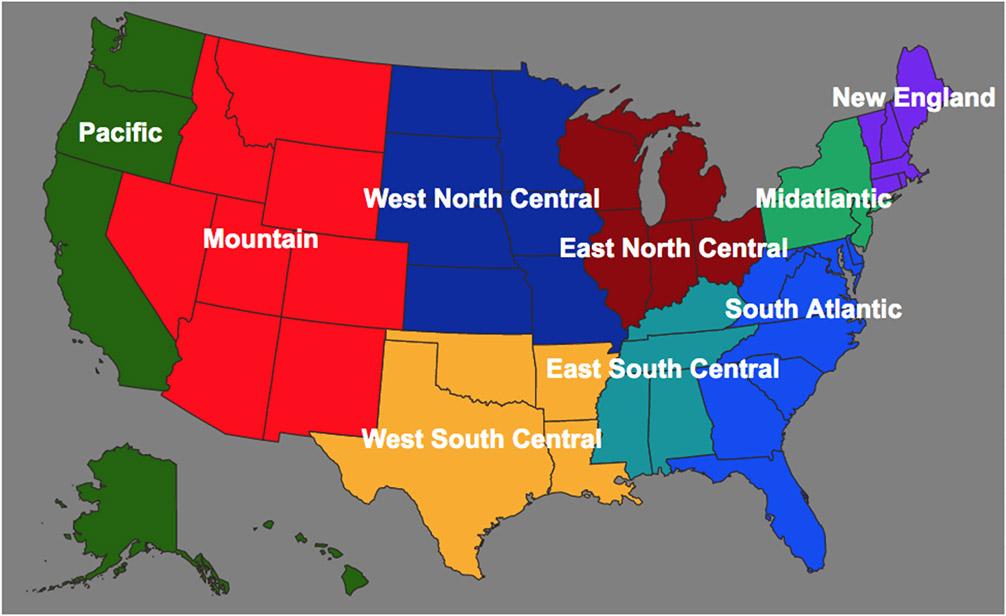
Results: A total of 48 787 patients were included. Survival was inferior in seven of nine regions for underinsured patients. In six regions survival was inferior for Medicaid and Medicare patients, respectively: Middle Atlantic: hazard ratio (HR) 1.25 and 1.22; South Atlantic: HR 1.41 and HR 1.22; East North Central: HR 1.36 and HR 1.25; East South Central: HR 1.37 and HR 1.25; West North Central: HR 1.67 and HR 1.42; West South Central: HR 1.44 and HR 1.46. In the Pacific region survival was inferior for Medicare patients (HR 1.35) but not inferior for Medicaid patients. Being uninsured was associated with worse survival in the South Atlantic (HR 1.23), East North Central (HR 1.23), East South Central (HR 1.56), and West South Central (HR 1.31) regions. Annual income level under $38 000 was associated with worse survival in the Middle Atlantic (HR 1.24), South Atlantic (HR 1.35), and East North Central (HR 1.49) regions. Lastly, when compared with academic research institutions, comprehensive community cancer centers had significantly worse survival in four of the nine regions.
Conclusions: Cervical cancer mortality is higher for women with a low income, underinsured (Medicaid or Medicare) or uninsured status, and decreased access to academic institutions in most US regions. An increase in cervical cancer mortality was associated with underinsured or uninsured populations in regions mainly located in the South and Midwest.
Keywords: Cervical Cancer; Cervix Uteri.
© IGCS and ESGO 2022. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Howlader NNA, Krapcho M, Miller D, eds. SEER Cancer Statistics Review. Bethesda, MD: National Cancer Institute, 1975–2017.
-
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33 - PubMed
-
- Lei J, Ploner A, Elfström KM, et al. HPV vaccination and the risk of invasive cervical cancer. N Engl J Med 2020;383:1340–8. - PubMed
