

The role of bile acids in carcinogenesis
- PMID: 35429253
- PMCID: PMC9013344
- DOI: 10.1007/s00018-022-04278-2
The role of bile acids in carcinogenesis
Abstract
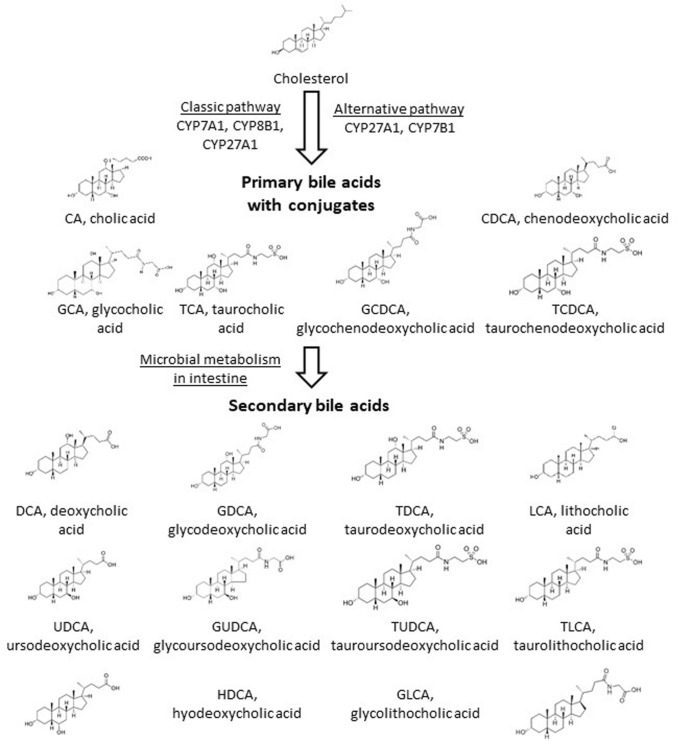
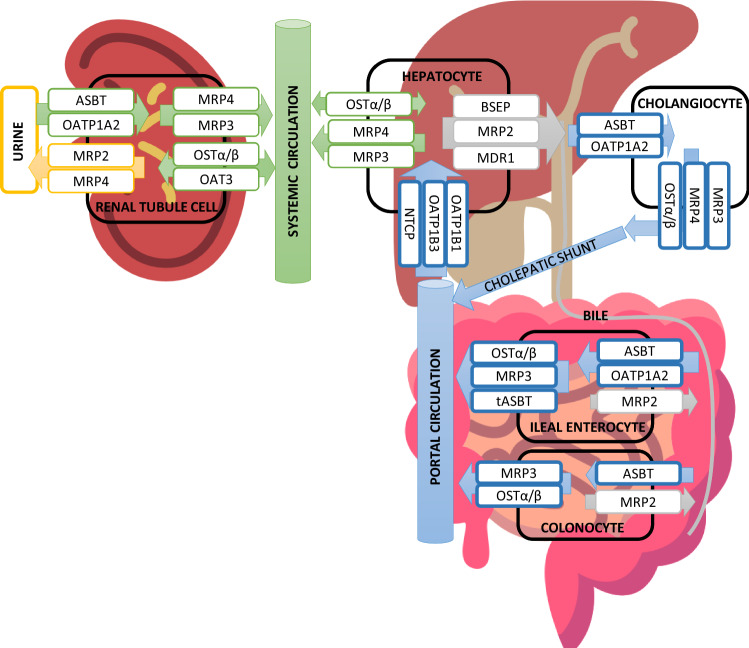
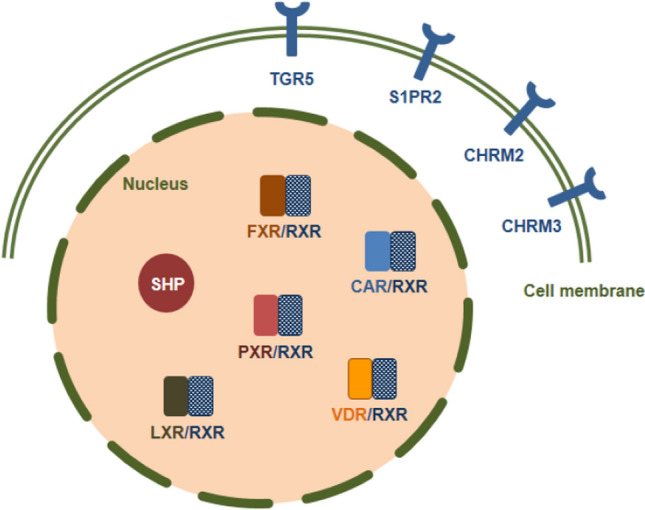
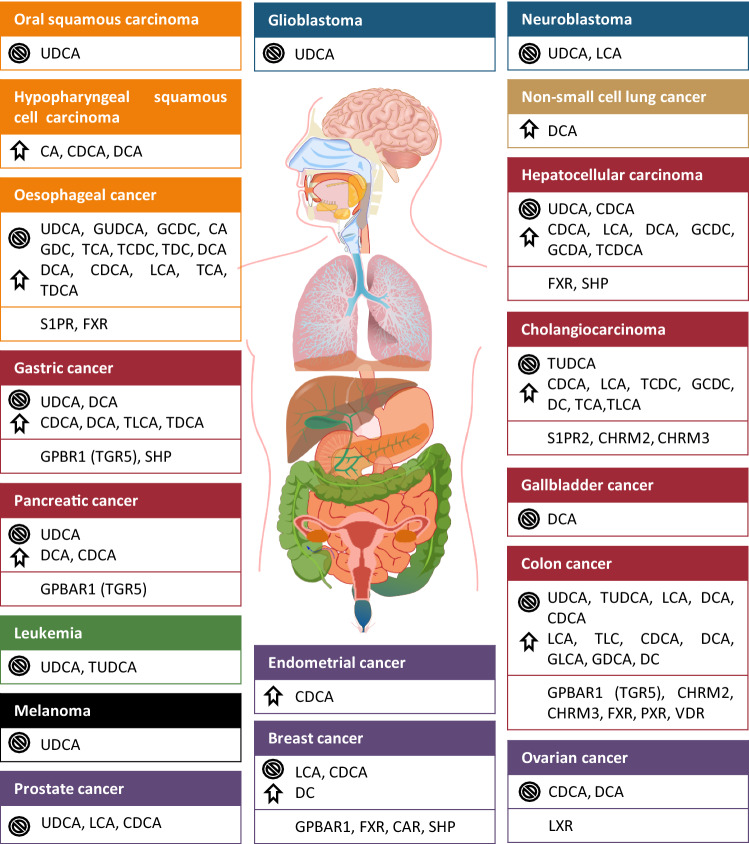
Bile acids are soluble derivatives of cholesterol produced in the liver that subsequently undergo bacterial transformation yielding a diverse array of metabolites. The bulk of bile acid synthesis takes place in the liver yielding primary bile acids; however, other tissues have also the capacity to generate bile acids (e.g. ovaries). Hepatic bile acids are then transported to bile and are subsequently released into the intestines. In the large intestine, a fraction of primary bile acids is converted to secondary bile acids by gut bacteria. The majority of the intestinal bile acids undergo reuptake and return to the liver. A small fraction of secondary and primary bile acids remains in the circulation and exert receptor-mediated and pure chemical effects (e.g. acidic bile in oesophageal cancer) on cancer cells. In this review, we assess how changes to bile acid biosynthesis, bile acid flux and local bile acid concentration modulate the behavior of different cancers. Here, we present in-depth the involvement of bile acids in oesophageal, gastric, hepatocellular, pancreatic, colorectal, breast, prostate, ovarian cancer. Previous studies often used bile acids in supraphysiological concentration, sometimes in concentrations 1000 times higher than the highest reported tissue or serum concentrations likely eliciting unspecific effects, a practice that we advocate against in this review. Furthermore, we show that, although bile acids were classically considered as pro-carcinogenic agents (e.g. oesophageal cancer), the dogma that switch, as lower concentrations of bile acids that correspond to their serum or tissue reference concentration possess anticancer activity in a subset of cancers. Differences in the response of cancers to bile acids lie in the differential expression of bile acid receptors between cancers (e.g. FXR vs. TGR5). UDCA, a bile acid that is sold as a generic medication against cholestasis or biliary surge, and its conjugates were identified with almost purely anticancer features suggesting a possibility for drug repurposing. Taken together, bile acids were considered as tumor inducers or tumor promoter molecules; nevertheless, in certain cancers, like breast cancer, bile acids in their reference concentrations may act as tumor suppressors suggesting a Janus-faced nature of bile acids in carcinogenesis.
Keywords: Bile acid; Bile acid biosynthesis; Bile acid receptors; Bile acid transporters; Breast cancer; CA; CAR; CDCA; Carcinogenesis; Colorectal carcinoma; DCA; Epithelial–mesenchymal transition; FXR; Gastric cancer; Hepatocellular carcinoma; LCA; LXR; Microbiome; Muscarinic receptor CHRM2; Muscarinic receptor CHRM3; Oesophageal carcinoma; Ovarian cancer; Oxidative stress; PXR; Pancreatic adenocarcinoma; Primary bile acid; Prostate cancer; S1PR2; SHP; Secondary bile acid; TGR5; UDCA; VDR; Warburg metabolism.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pellicciari R, Gioiello A, Costantino G. Potential therapeutic applications of farnesoid X receptor (FXR) modulators. Expert Opin Ther Pat. 2006;16:333–341. doi: 10.1517/13543776.16.3.333. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
