

The association of intensity and duration of non-pharmacological interventions and implementation of vaccination with COVID-19 infection, death, and excess mortality: Natural experiment in 22 European countries
- PMID: 35429788
- PMCID: PMC8944114
- DOI: 10.1016/j.jiph.2022.03.011
The association of intensity and duration of non-pharmacological interventions and implementation of vaccination with COVID-19 infection, death, and excess mortality: Natural experiment in 22 European countries
Abstract
Background: Critical questions remain regarding the need for intensity to continue NPIs as the public was vaccinated. We evaluated the association of intensity and duration of non-pharmaceutical interventions (NPIs) and vaccines with COVID-19 infection, death, and excess mortality in Europe.
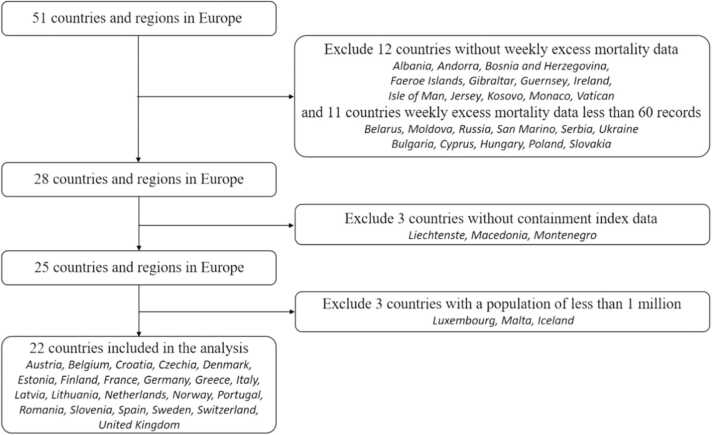
Methods: Data comes from Our Word in Data. We included 22 European countries from January 20, 2020, to May 30, 2021. The time-varying constrained distribution lag model was used in each country to estimate the impact of different intensities and duration of NPIs on COVID-19 control, considering vaccination coverage. Country-specific effects were pooled through meta-analysis.
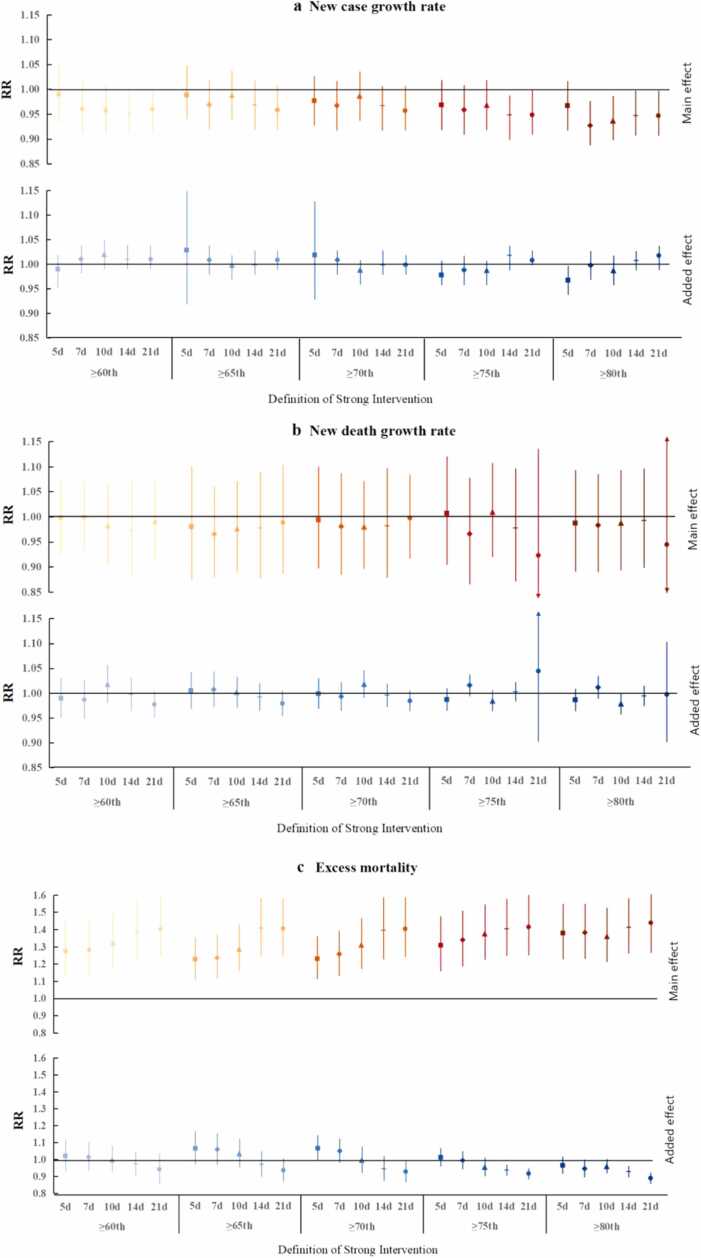
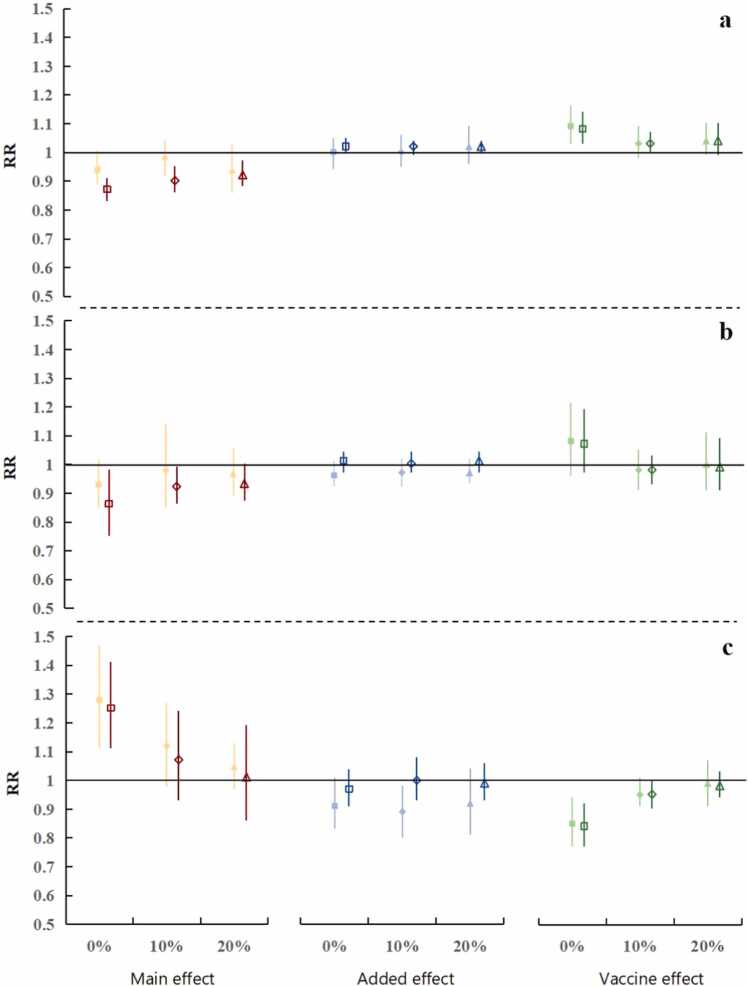
Results: This study found that high-intensity and long-duration of NPIs showed a positive main effect on reducing infection in the absence of vaccines, especially in the intensity above the 80th percentile and lasted for 7 days (RR = 0.93, 95% CI: 0.89-0.98). However, the adverse effect on excess mortality also increased with the duration and intensity. Specifically, it was associated with an increase of 44.16% (RR = 1.44, 95% CI: 1.27-1.64) in the excess mortality under the strict intervention (the intensity above the 80th percentile and lasted for 21 days). As the vaccine rollouts, the inhibition of the strict intervention on cases growth rate was increased (RR dropped from 0.95 to 0.87). Simultaneously, vaccination also alleviated the negative impact of the strict intervention on excess mortality (RR decreased from 1.44 to 1.25). Besides, maintaining the strict intervention appeared to more reduce the cases, as well as avoids more overall burden of death compared with weak intervention.
Conclusions: Our study highlights the importance of continued high-intensity NPIs in low vaccine coverage. Lifting of NPIs in insufficient vaccination coverage may cause increased infections and death burden. Policymakers should coordinate the intensity and duration of NPIs and allocate medical resources reasonably with widespread vaccination.
Keywords: COVID-19; Dynamic intervention; Excess mortality; Non-pharmacological interventions; Time series analysis; Vaccine.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Competing interests The authors declare no competing financial interests.
Figures
Similar articles
-
Non-pharmaceutical interventions in containing COVID-19 pandemic after the roll-out of coronavirus vaccines: a systematic review.BMC Public Health. 2024 Jun 6;24(1):1524. doi: 10.1186/s12889-024-18980-2. BMC Public Health. 2024. PMID: 38844867 Free PMC article.
-
Association of Simulated COVID-19 Vaccination and Nonpharmaceutical Interventions With Infections, Hospitalizations, and Mortality.JAMA Netw Open. 2021 Jun 1;4(6):e2110782. doi: 10.1001/jamanetworkopen.2021.10782. JAMA Netw Open. 2021. PMID: 34061203 Free PMC article.
-
Vaccination as an alternative to non-drug interventions to prevent local resurgence of COVID-19.Infect Dis Poverty. 2022 Mar 26;11(1):36. doi: 10.1186/s40249-022-00960-6. Infect Dis Poverty. 2022. PMID: 35346382 Free PMC article.
-
COVID-19 case doubling time associated with non-pharmaceutical interventions and vaccination: A global experience.J Glob Health. 2021 Sep 4;11:05021. doi: 10.7189/jogh.11.05021. eCollection 2021. J Glob Health. 2021. PMID: 34552726 Free PMC article.
-
Comparison of COVID-19 and seasonal influenza under different intensities of non-pharmaceutical interventions and vaccine effectiveness.Front Public Health. 2022 Sep 27;10:973088. doi: 10.3389/fpubh.2022.973088. eCollection 2022. Front Public Health. 2022. PMID: 36238257 Free PMC article. Review.
Cited by
-
The added effect of non-pharmaceutical interventions and lifestyle behaviors on vaccine effectiveness against severe COVID-19 in Chile: A matched case-double control study.Vaccine. 2023 May 2;41(18):2947-2955. doi: 10.1016/j.vaccine.2023.03.060. Epub 2023 Apr 3. Vaccine. 2023. PMID: 37024408 Free PMC article.
-
Global trends in COVID-19 incidence and case fatality rates (2019-2023): a retrospective analysis.Front Public Health. 2024 Jul 29;12:1355097. doi: 10.3389/fpubh.2024.1355097. eCollection 2024. Front Public Health. 2024. PMID: 39135930 Free PMC article.
-
A global analysis of COVID-19 infection fatality rate and its associated factors during the Delta and Omicron variant periods: an ecological study.Front Public Health. 2023 Jun 2;11:1145138. doi: 10.3389/fpubh.2023.1145138. eCollection 2023. Front Public Health. 2023. PMID: 37333556 Free PMC article.
-
Non-pharmaceutical interventions in containing COVID-19 pandemic after the roll-out of coronavirus vaccines: a systematic review.BMC Public Health. 2024 Jun 6;24(1):1524. doi: 10.1186/s12889-024-18980-2. BMC Public Health. 2024. PMID: 38844867 Free PMC article.
-
The rapid and efficient strategy for SARS-CoV-2 Omicron transmission control: analysis of outbreaks at the city level.Infect Dis Poverty. 2022 Nov 24;11(1):114. doi: 10.1186/s40249-022-01043-2. Infect Dis Poverty. 2022. PMID: 36434701 Free PMC article.
References
-
- World Health Organization. WHO Director-General's opening remarks at the media briefing on COVID-19 – 11 March 2020. [cited 2020 March 12]. Available from: 〈https://www.who.int/dg/speeches/detail/who-director-general-s-opening-r....
-
- WHO. WHO Coronavirus (COVID-19) Dashboard. World Health Organization. WHO coronavirus disease (COVID-19) dashboard; 2022. [cited 2022 March 8]. Available from: 〈https://covid19.who.int〉.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
