

Extracolonic findings at CT colonography in an oncological hospital setting and why they matter
- PMID: 35429830
- PMCID: PMC9432346
- DOI: 10.1016/j.clinimag.2022.03.020
Extracolonic findings at CT colonography in an oncological hospital setting and why they matter
Abstract
Purpose: To evaluate the frequency and clinical outcome of unknown extracolonic findings in patients with cancer who underwent CT colonography (CTC).
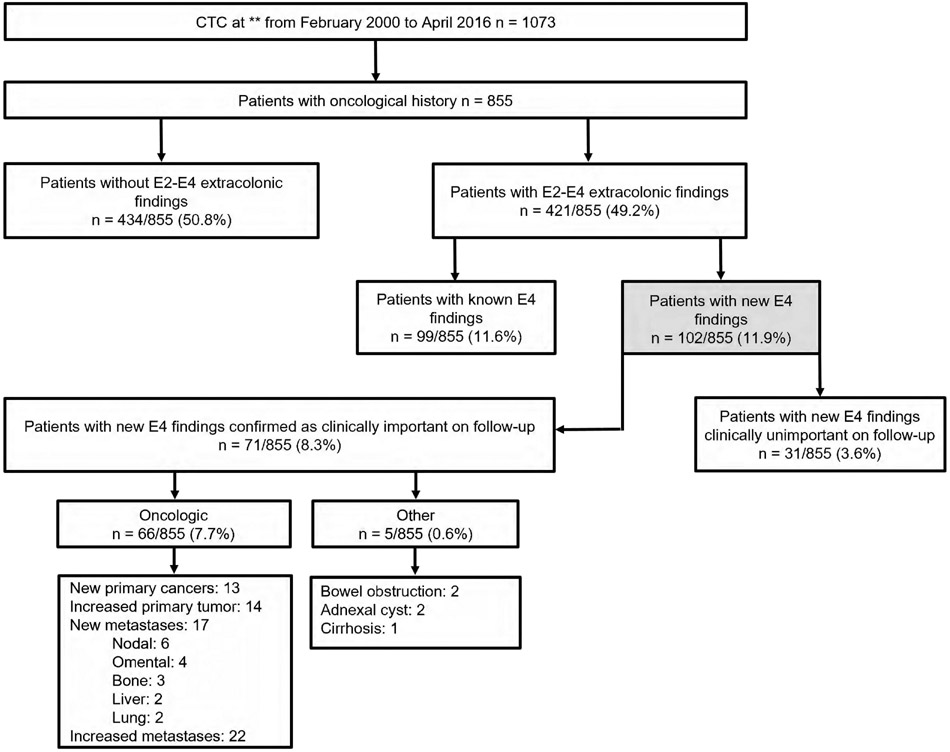
Methods: Consecutive patients who underwent CTC from February 2000-April 2016 for any indication were retrospectively included. One radiologist blinded to clinical data determined C-RADS classification for all extracolonic findings on CTC reports as follows: E1: normal examination or anatomic variant, E2: clinically unimportant, E3: likely unimportant, incompletely characterized, and E4: potentially important. Another radiologist performed an unblinded review of medical records and determined if E4 findings were previously known or new, and classified new E4 findings as clinically important or unimportant on follow-up.
Results: Of 855 patients, 686/855 (80.2%) had a normal examination or clinically unimportant extracolonic findings (E1 and E2) and 169/855 (19.8%) had E3-E4 extracolonic findings [99/855 (11.6%) patients had known E4 findings and 102/855 (11.9%) patients had new E4 findings]. On follow-up, among new E4 findings, 71/855 (8.3%) patients had clinically important findings, 66/855 (7.7%) had a malignant outcome previously unknown by the referring physician, and 5/855 (0.6%) had other complications, including bowel obstruction and cirrhosis. Regarding new oncological findings, new extracolonic primary tumors were detected in 13/855 (1.5%) patients, corresponding to 12.7% (13/102) of the new E4 findings. The proportion of new E4 findings on CTC with and without intravenous contrast was not significantly different [41/320 (12.8%) vs 61/535 (11.4%), p = 0.612].
Conclusion: Among oncological patients, detection of new significant E4 extracolonic findings at CTC occurred in 8.3% of all cases, including unknown cancers in 1.5%.
Keywords: CT colonography; Incidental findings; Tomography; cancer care facilities.
Copyright © 2022. Published by Elsevier Inc.
Conflict of interest statement
Figures
Similar articles
-
Comparison of extracolonic findings and clinical outcomes in a screening and diagnostic CT colonography population.Abdom Radiol (NY). 2019 Feb;44(2):429-437. doi: 10.1007/s00261-018-1753-3. Abdom Radiol (NY). 2019. PMID: 30209542 Free PMC article.
-
Potentially Important Extracolonic Findings at Screening CT Colonography: Incidence and Outcomes Data From a Clinical Screening Program.AJR Am J Roentgenol. 2016 Feb;206(2):313-8. doi: 10.2214/AJR.15.15193. Epub 2015 Oct 22. AJR Am J Roentgenol. 2016. PMID: 26491809 Free PMC article.
-
Indeterminate but Likely Unimportant Extracolonic Findings at Screening CT Colonography (C-RADS Category E3): Incidence and Outcomes Data From a Clinical Screening Program.AJR Am J Roentgenol. 2016 Nov;207(5):996-1001. doi: 10.2214/AJR.16.16275. Epub 2016 Aug 9. AJR Am J Roentgenol. 2016. PMID: 27505184 Free PMC article.
-
JOURNAL CLUB: Extracolonic Findings at CT Colonography: Systematic Review and Meta-Analysis.AJR Am J Roentgenol. 2018 Jul;211(1):25-39. doi: 10.2214/AJR.17.19495. Epub 2018 May 24. AJR Am J Roentgenol. 2018. PMID: 29792744
-
Extracolonic findings at CT colonography.Gastrointest Endosc Clin N Am. 2010 Apr;20(2):305-22. doi: 10.1016/j.giec.2010.02.013. Gastrointest Endosc Clin N Am. 2010. PMID: 20451819 Review.
References
-
- U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2013 Incidence and Mortality Web-based Report., www.cdc.gov/uscs.; 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
