

Targeting oncometabolism to maximize immunotherapy in malignant brain tumors
- PMID: 35430605
- PMCID: PMC9081266
- DOI: 10.1038/s41388-022-02312-y
Targeting oncometabolism to maximize immunotherapy in malignant brain tumors
Abstract
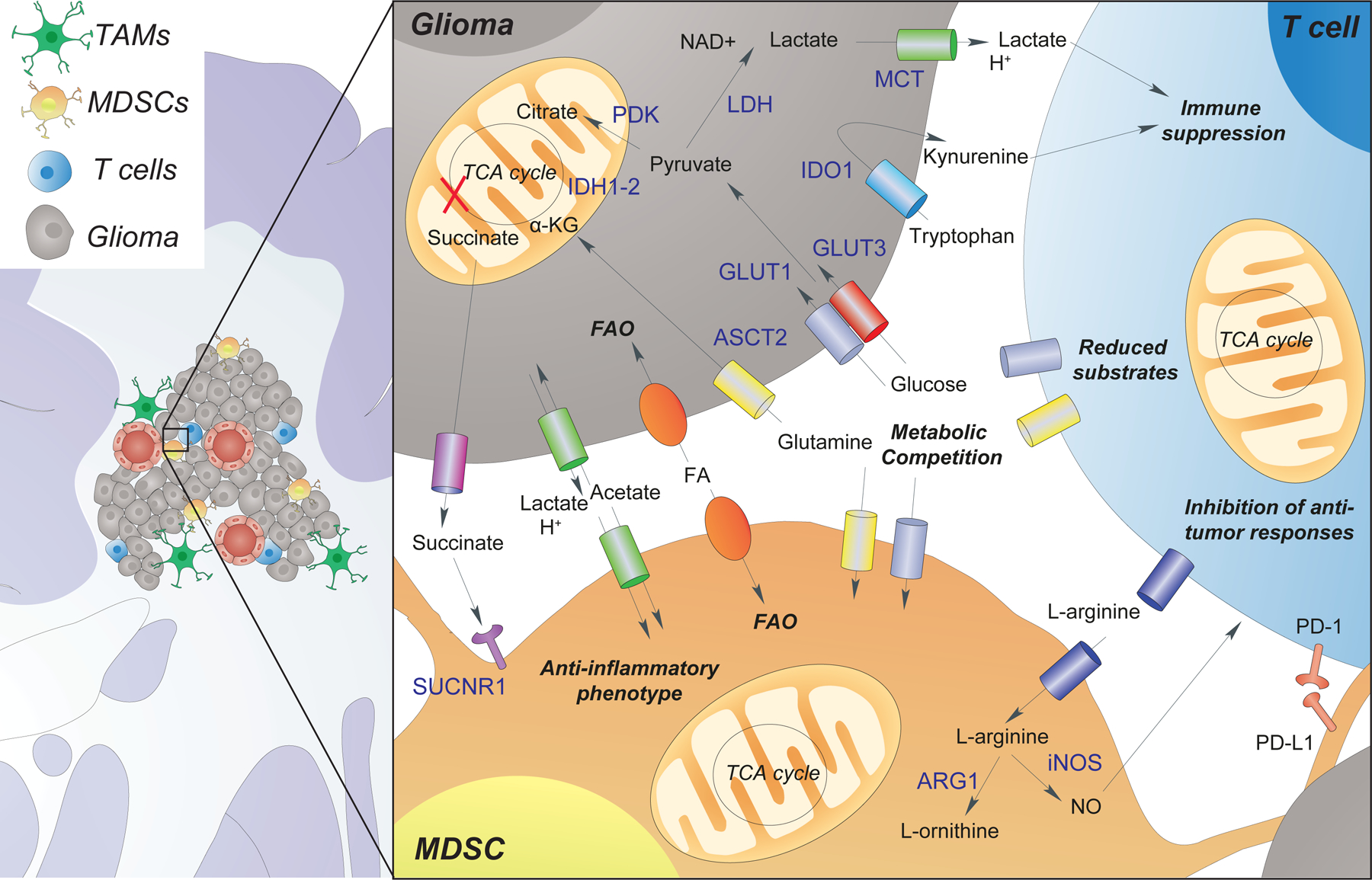
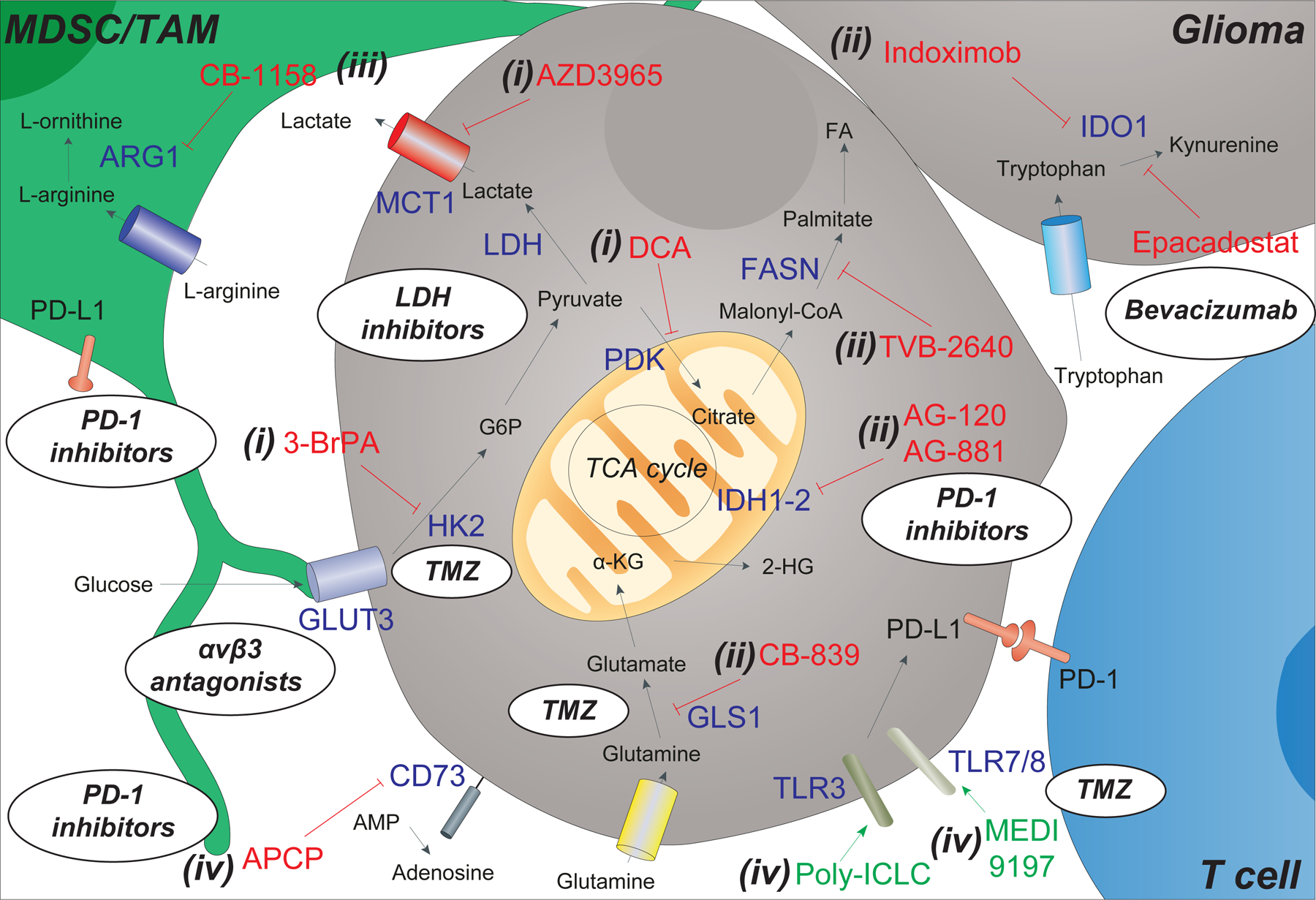
Brain tumors result in significant morbidity and mortality in both children and adults. Recent data indicate that immunotherapies may offer a survival benefit after standard of care has failed for malignant brain tumors. Modest results from several late phase clinical trials, however, underscore the need for more refined, comprehensive strategies that incorporate new mechanistic and pharmacologic knowledge. Recently, oncometabolism has emerged as an adjunct modality for combinatorial treatment approaches necessitated by the aggressive, refractory nature of high-grade glioma and other progressive malignant brain tumors. Manipulation of metabolic processes in cancer and immune cells that comprise the tumor microenvironment through controlled targeting of oncogenic pathways may be utilized to maximize the efficacy of immunotherapy and improve patient outcomes. Herein, we summarize preclinical and early phase clinical trial research of oncometabolism-based therapeutics that may augment immunotherapy by exploiting the biochemical and genetic underpinnings of brain tumors. We also examine metabolic pathways related to immune cells that target tumor cells, termed "tumor immunometabolism". Specifically, we focus on glycolysis and altered glucose metabolism, including glucose transporters, hexokinase, pyruvate dehydrogenase, and lactate dehydrogenase, glutamine, and we discuss targeting arginase, adenosine, and indoleamine 2,3-dioxygenase, and toll-like receptors. Lastly, we summarize future directions targeting metabolism in combination with emerging therapies such as oncolytic virotherapy, vaccines, and chimeric antigen receptor T cells.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Figures
References
-
- Rogers TW, Toor G, Drummond K, Love C, Field K, Asher R et al. The 2016 revision of the WHO Classification of Central Nervous System Tumours: retrospective application to a cohort of diffuse gliomas. J Neurooncol 2018; 137: 181–189. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJB et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl J Med 2005; 352: 987–996. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
